PCR - A critical examination
translated by Corona InvestigativeHere ← Back to page 1
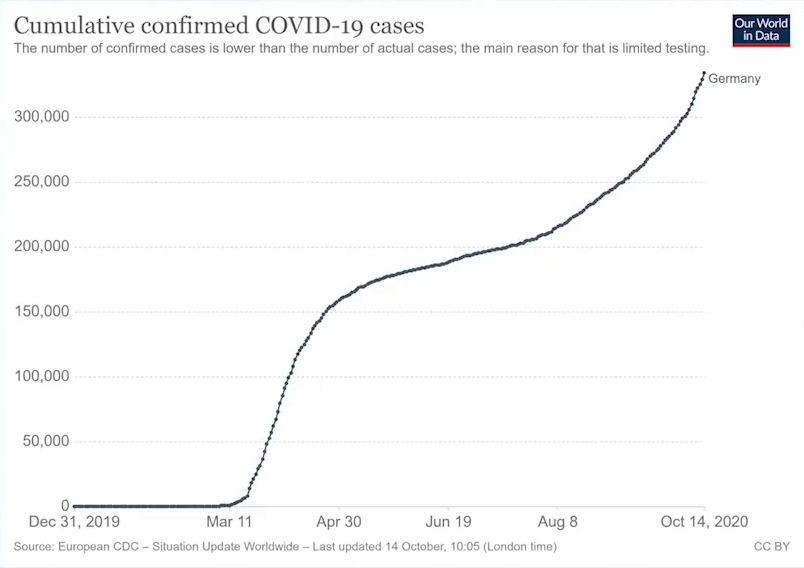
In this chart above we see the cumulative numbers of positive test results, commonly referred to as infected, more clearly. You can see how the numbers are decreasing after the initial mass hysteria, but then increase rapidly at the beginning of August with the second wave of tests. It is also not surprising that there are more cases of colds at the beginning of autumn. This is the case every year.
In the case of a cold, dead cell material is excreted from the lungs and throat by mouth and nose. As mentioned earlier in this article, the probability of a test being considered positive varies depending on where the sample is collected. The probability is greatly increased for mucus from the throat or lungs. If this mucus is in the nose and mouth due to a cold, you will find many more cell fragments that contain huge amounts of all kinds of RNA and can therefore make PCR tests positive. If it is true that the tests do not show any correlation with real illnesses, then this should also be shown by the actual illnesses and death rates.
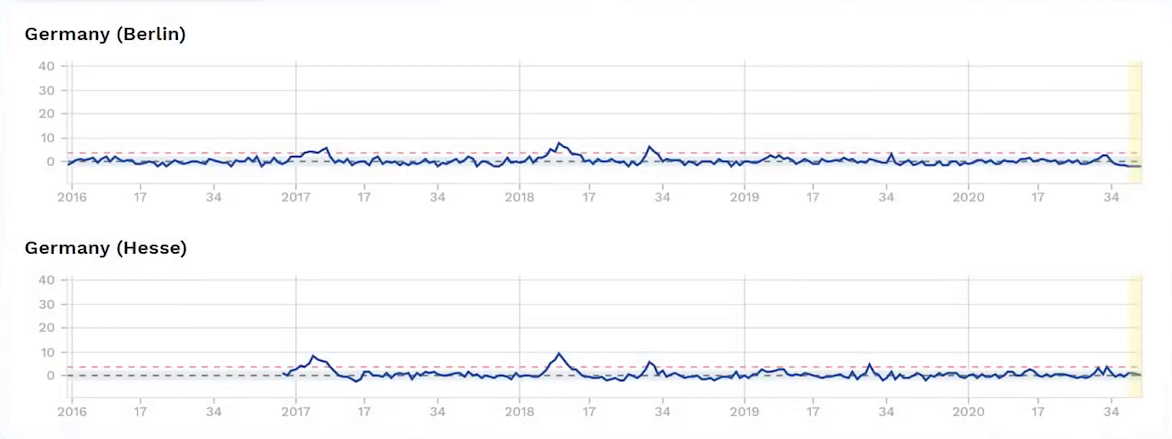
In the following graphic, we first look at the death figures for Germany as they can be viewed at EuroMomo. It becomes clear that there was no excess mortality in Germany this year (2020).
And the illness figures? Let's take a look at the data from the Robert Koch Institute (RKI) on acute respiratory diseases, which include the alleged pneumonia COVID-19.
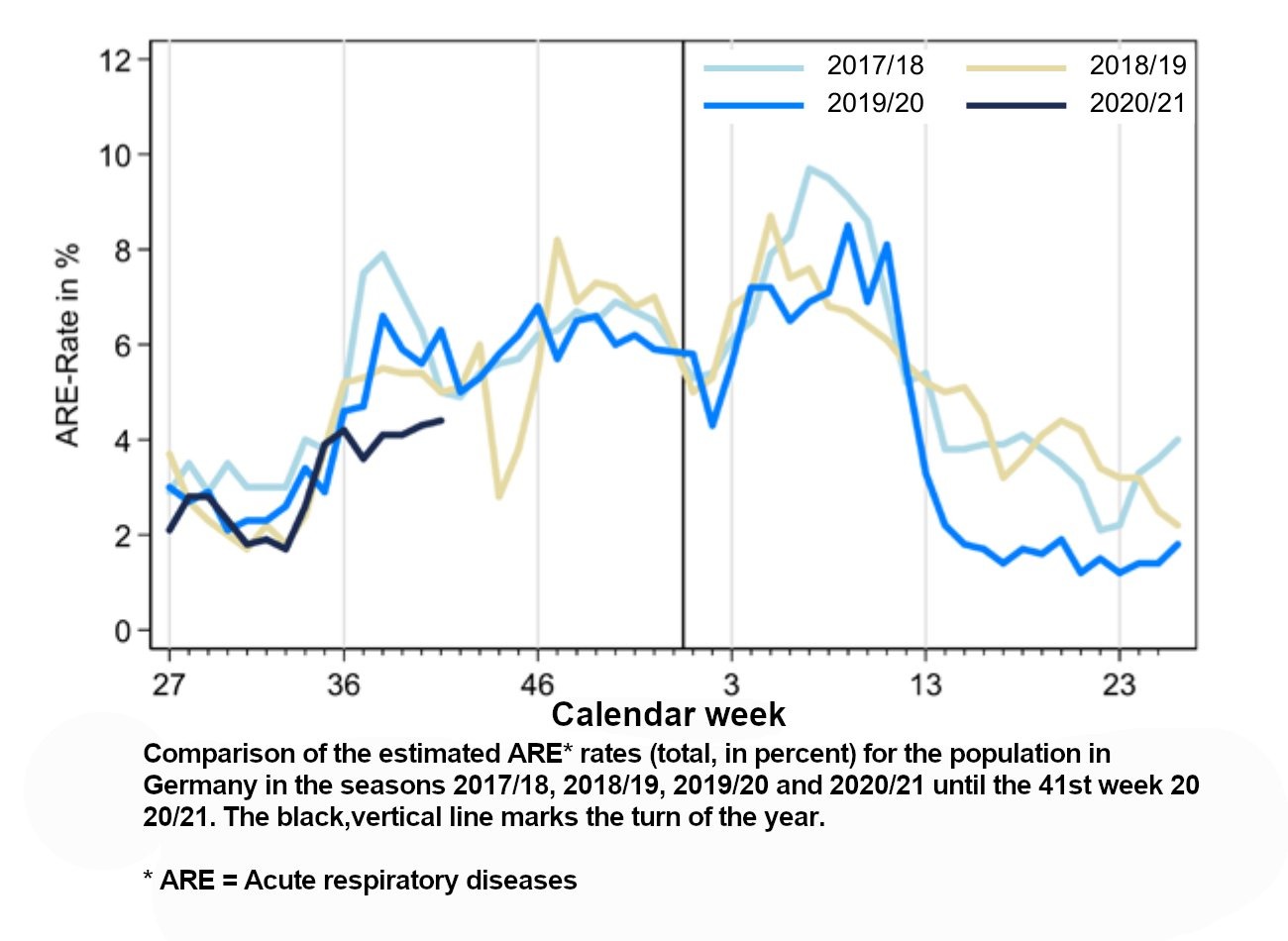
We recognize that the number of actual respiratory diseases is currently much lower than in the last three years. This confirms that the PCR results, which were evaluated as positive, have nothing to do with real cases of disease. This once again makes it clear that the results are probably false positives.
If we look (see graph down below) at the severe acute respiratory infections, or " Sari" for short, over the last few years, we see that 2020 was a very mild year for all age groups. Where are the additional 330,000 cases that are expected to occur as a result of the alleged pandemic that have tested positive? It becomes obvious that the number of so-called infected cases is of no significance at all. It has nothing to do with actual infections, because in 2020 these will be more rare than they have been for a long time.

CONCLUSION
According to the manufacturers of the components, the actual PCR process, this production technique, is therefore not suitable for medical diagnostic procedures. Even the inventor of the PCR, the biochemist Karry Mullis, who received the Nobel Prize for Chemistry, not the Nobel Prize for Medicine, in 1993, repeatedly refused to use this method in medical diagnostics. In particular, he was concerned with the use of his method in HIV testing, which was a particular topic in the 1990s. Let's listen (27) to what Mullis had to say about PCR testing at the time:
Audience Question: "How did they misuse PCR to estimate all the supposed free viral RNAs that may or may not be there."
Karry Mullis: "I think misuse PCR is not quiet... I don't think you can misuse PCR. The results, the interpretation, see... If they can find this virus in you at all, and the PCR if you do it well, you can find almost anything in anybody that starts making you void. In sort of Buddhist notion, that everything is contained in everything else. Right? I mean, if you can amplify one single molecule up to so much that you can really measure it, which PCR can do, then there is very few molecules that you don't have. At least single on of them in your body. Okay? So that could be thought of as a misuse just to claim that it is meaningful."
To the question whether the pure PCR provides estimates:
Karry Mullis: "It is not an estimation it is really a quantitative thing. It tells you something about nature and about what's there but it allows you to take a very miniscule amount of anything and make it measurable and then talk about it in meetings and with staff like it is important. That is not a misuse that is a sort of misinterpretation."
To establish that a so-called virus is only found in a tiny fraction of cells:
Karry Mullis: "The measurement for it, is not exact at all. It is not as good as I measure things like apples. An apple is an apple. You can get something....If you get enough things that look like a kind of apple and you stick em all together, you might think that it is an apple. But... and HIV is like that. It is all based on things that are invisible and the results are inferred. PCR is separat from that. It is just a process that is used to make a whole lot of something out of something. It doesn't tell you that you are sick and it doesn't tell you that the thing you ended up with, really was gonna hurt you."
The pure PCR is only a very error-prone DNA duplication technique which, as we have heard, can detect everything in anyone. Mullis was always skeptical about the interpretation of the test results. He doubted that any highly amplified gene sequence had any significance for a person's health, which is why he rejected diagnostic PCR tests. He told the New York Times in 1998:
"Scientist are doing an awful lot of damage to the world in the name of helping it. I don't mind attacking my own fraternity because I am ashamed of it," Dr. Mullis says.
The scientists have brought the world to the brink of collapse with their blind faith in an impotent and meaningless test. They have damaged millions upon millions of lives, destroyed existences. It is time for the medical profession, associations and societies to stand up and take up the cudgels for purely clinical diagnosis and against any form of indiscriminate mass testing with tests that give nothing but misinterpreted results. At the end of September, the Austrian Medical Association (28) took a cautious step in the right direction when it issued the following statement:
"The more I test, the more I will generate positive test results. And the less significant they are, and you just have to see which of them really gets sick and which ends up in intensive care, and this number doesn't increase nearly proportionally to the number of tests that are performed. In addition, this huge number of tests is only possible if institutions are created specifically to do this, which are not created according to the recognized rules of medicine and the necessary guidelines regarding quality." [...] "Tests without subsequent diagnosis by a physician are not really suitable to be sure of COVID-19 disease." [...] "If you do not know whether the person is asymptomatic or has a cold, sore throat, fever or pneumonia, then this is the result of limited value."
This is how it must continue. It is high time that all doctors, scientists and medical associations worldwide wake up from their lethargy and take a clear stand against mass testing and put an end to this madness. And as far as a conclusion about the PCR tests is concerned, this should not come from me, but from Professor Dr. Stephen Bustin.
Due to the complete lack of strict guidelines for the performance of PCR tests, he tried to introduce such guidelines (29) under the term MIQE (Minimum Information for Publication of Quantitative Real-Time PCR Experiments) in 2009 and insisted on their strict compliance. Eight years later, in 2017, he was dismayed to find that the MIQE was not being implemented:
"Poorly executed and inadequately reported molecular measurement methods are amongst the causes underlying the lack of reproducibility of much biomedical research. Although several high impact factor journals have acknowledged their past failure to scrutinise adequately the technical soundness of manuscripts, there is a perplexing reluctance to implement basic corrective measures. The reverse transcription real‐time quantitative PCR (RT‐qPCR) is probably the most straightforward measurement technique available for RNA quantification and is widely used in research, diagnostic, forensic and biotechnology applications. Despite the impact of the minimum information for the publication of quantitative PCR experiments (MIQE) guidelines, which aim to improve the robustness and the transparency of reporting of RT‐qPCR data, we demonstrate that elementary protocol errors, inappropriate data analysis and inadequate reporting continue to be rife and conclude that the majority of published RT‐qPCR data are likely to represent technical noise."
That the world's leading expert in the field of qPCR, who believes that the majority of PCR data from research, where work is much more conscientious than in current rapid tests, is no more than a rush, destroys the entire practice of PCR as a diagnostic procedure and takes the last remaining confidence that one might have had in the reliability of these tests. They are useless and highly dangerous as mass tests. Or as the epidemiologist Prof. Dr. Ulrike Kämmerer recently said in an interview (30) with the lawyer Dr. Reiner Fuellmich in the German Corona Committee:
Dr. Fuellmich: "If I have not completely misunderstood this, it is that all the positive tests, in truth, say nothing about whether these negative people tested are actually infected or sick."
Dr. Kämmerer: "That is correct. [...] This is simply a problem where you set the so-called cut-off. This is usually not defined in the works. This qCT value, so they say, must be specified. It will never be announced with which PCR and under which conditions these positive results will be obtained. Therefore it is absolutely not possible to evaluate what is output. It is like reading coffee grounds."
There are only two reasons why experts like Christian Drosten, who should undoubtedly know about the error-proneness and unreliability of the system, fail to address this issue clearly. Either they are really not aware of it, in which case they would be dangerously incompetent, or they know about it but conceal it. Then they would be criminally irresponsible. In the end, the world, led by a few panicky molecular biologists and virologists, has let itself be kidnapped by a technology that, even after 35 years, does not control it, perhaps even does not really understand it. A public review is urgently needed and the tests must be stopped immediately. These dashboards of state health departments, which graphically and impressively list the alleged COVID-19 cases by state, are an expression of an illusory world without any real worldly significance for people's health. It is only empty numbers bungled together on basis of wrong mass tests. Only statistics based on real death figures and the assessments of family doctors reflect the true situation. We need to return to clinical diagnosis of people who actually suffer from pneumonia, which is the same number as it has been for the past tens of years. Let us recall the New York Times article (31) on Darthmouth. "Trust in Corona Quick Test leads to Epidemic That Wasn’t."
Transcribed, translated and adapted Version - Original video here
Back to the main page of this Telegraph blog: Link
Visit our Telegram Channel for additional news & information: Link
Chat with like-minded in our Telegram Chat Group: Link
Please support to keep this blog alive: paypal
References & notes:
(1) Performance evaluation of thermal cyclers for PCR in a rapid cycling condition
(2) Individual EUAs for Molecular Diagnostic Tests for SARS-CoV-2
(3) Thermo Fisher website search result for Thermocycler. Scroll down to bottom to see the note
(4) PfuTurbo Cx HotStart DNA Polymerase
(5) Titanium Taq SP—high-yield DNA polymerase for laboratory testing (GPR-registered)
(6) Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR
(7) SuperScript™ III One-Step RT-PCR System with Platinum™ Taq DNA Polymerase
(8) TaqMan™ Fast Virus 1-Step Master Mix
(9) Detection of SARS-CoV-2 in Different Types of Clinical Specimens
(10) Which RNA Isolation Kit is Right for Your qRT-PCR Experiment?
(11) Epidemiologic Features and Clinical Course of Patients Infected With SARS-CoV-2 in Singapore
(12) PCR Cycling Parameters–Six Key Considerations for Success
(13) The Infectious Myth - Stephen Bustin on Challenges with RT-PCR
(14) PCR Calculator
(15) EUA Authorized Serology Test Performance
(16) Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR
(17) Interpreting a covid-19 test result
(18) Potential false-positive rate among the 'asymptomatic infected individuals' in close contacts of COVID-19 patients
(19) Faith in Quick Test leads to Epidemic That Wasn't
(20) ABC TV interview Australian infectious disease specialist Sanjaya
(21) see 17
(22) False-negative results of initial RT-PCR assays for COVID-19: A systematic review
(23) Diagnosing COVID-19 infection: the danger of over-reliance on positive test results
(24) Report on Extra External Quality Assessment Scheme Group No. 340 Virus Genome Detection – SARS-CoV-2
(25) WHO Director-General's opening remarks at the media briefing on COVID-19 - 16 March 2020
(26) see 9
(27) Kary Mullis, inventor of the PCR, talks about the HIV-AIDS connection
(28) Österreichische Ärztekammer - „Schluss mit Corona Panik“ (Austrian Medical Association - "Stop Corona Panic")
(29) The MIQE guidelines: minimum information for publication of quantitative real-time PCR experiments
(30) Stiftung Corona-Ausschuss 4: Prof. Dr. Ulrike Kämmerer und Dr. Wolfgang Wodarg (Foundation Corona Committee 4: Prof. Dr. Ulrike Kämmerer and Dr. Wolfgang Wodarg)
(31) see 19