The more tests, the less basic rights... Statistics for advanced users
translated by Corona InvestigativeUpdate 29.07.2020: And again, the RKI provides a prime example for a (formulated in a value-free manner) not unproblematic handling of the numbers generated by himself - Lothar Wieler is "concerned about rising infection numbers" (DLF 28.07.2020), which we still do not know in Germany. Also Wieler only knows the numbers of positive test results - they are actually increasing, but so is the number of tests performed, and they are increasing massively (see below)... .
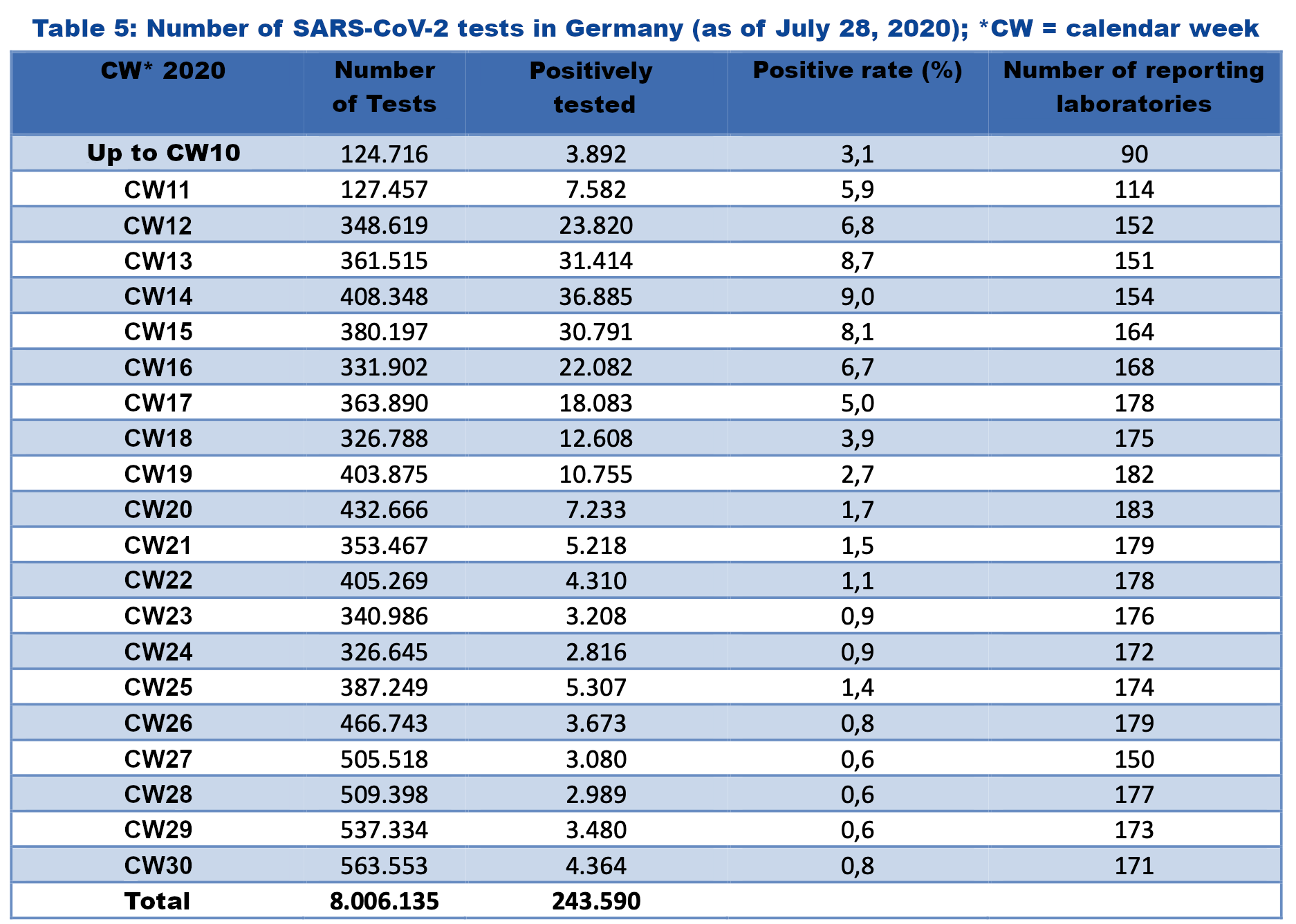
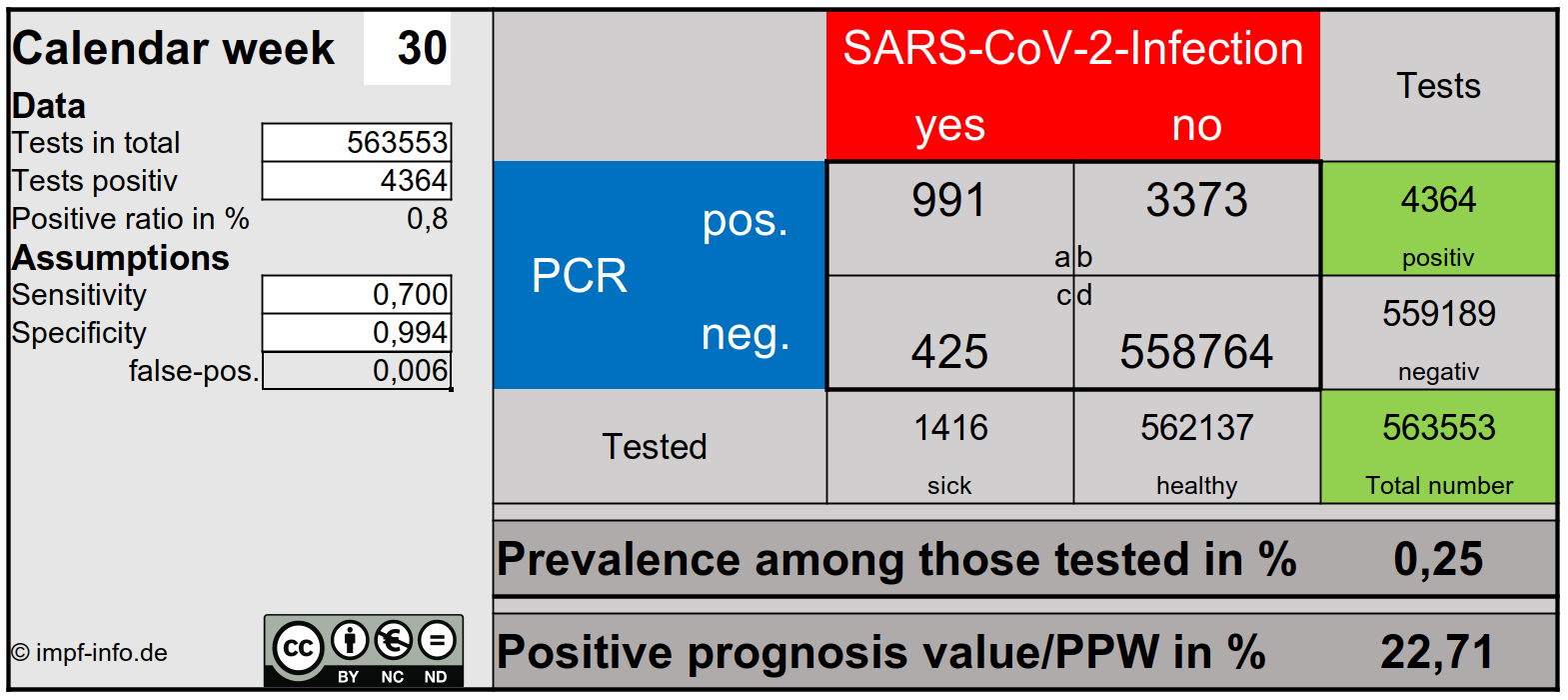
The portion of positive test results of their total number rose in the week 30 nevertheless slightly, lies thereby in addition, only so highly, as before approximately 4 weeks and measured at international yardsticks in the ultra-green range...
And the probability that a positive test result actually means an infection is still low: only about one in five positive tests actually shows COVID-19 correctly...
(Source: RKI Situation Report 29.07.2020)
Update 23.07.2020:
With the specificity from the INSTAND interlaboratory comparison (see below) of 99.3%, it is still not possible to calculate meaningful figures - a publication from June, in which Christian Drosten, among others, participated and which examined the specificity of RT-PCR under conditions of "real" (laboratory) life (Matheeussen 2020), resulted in a false positive rate of 0.58%. If this is taken as a basis, the above figures are obtained.
But of course, the same applies to the RKI as the Bavarian LGL freely admitted: whether testing is done with one or two targets, whether positive results are cross-checked... All this is not known in Berlin at the RKI as well as in Erlangen at the LGL.
Update 28.06.2020: Meanwhile, the total positive test results of RT-PCR are regionally so low that they cannot be brought into agreement with the specificity of the INSTAND interlaboratory test (99.3%) - what can be the reason for this?
RT-PCR can in principle detect two different gene sequences ("targets") for SARS-CoV-2 and, if both sequences are detected in one sample, achieves specificities of almost 100%.
However, in a publication of March 19, 2020, the WHO has decreed for regions affected by the pandemic that the detection of only one of the targets is sufficient for the sample to be found "positive": "In areas where COVID-19 virus is widely spread a simple algorithm might be adopted in which, for example, screening by rRT-PCR of a single discriminatory target is considered sufficient. (WHO 19.03.2020) This results - due to the missing double determination - naturally in a significantly lower specificity and thus a significantly higher rate of false-positive results.
This generous offer of the WHO was of course accepted by numerous laboratories (fewer determinations means: less costs), the MVZ Augsburg even got an article in an Austrian newspaper (Wochenblick 17.05.2020) via its blog entry of 03.04. (the entry has been deleted from the laboratory's blog in the meantime, but was definitely still there on 18.05.)
It is not known how many laboratories issue positive results for the detection of one target, how many determine both targets from the beginning and how many at least positive tests with one target are then checked with the other (retesting as described in the article of the NZZ below) - this double determination or retesting obviously increases the specificity relevantly beyond 99.3%.
To which value? Here RKI, PEI & Co are silent... .
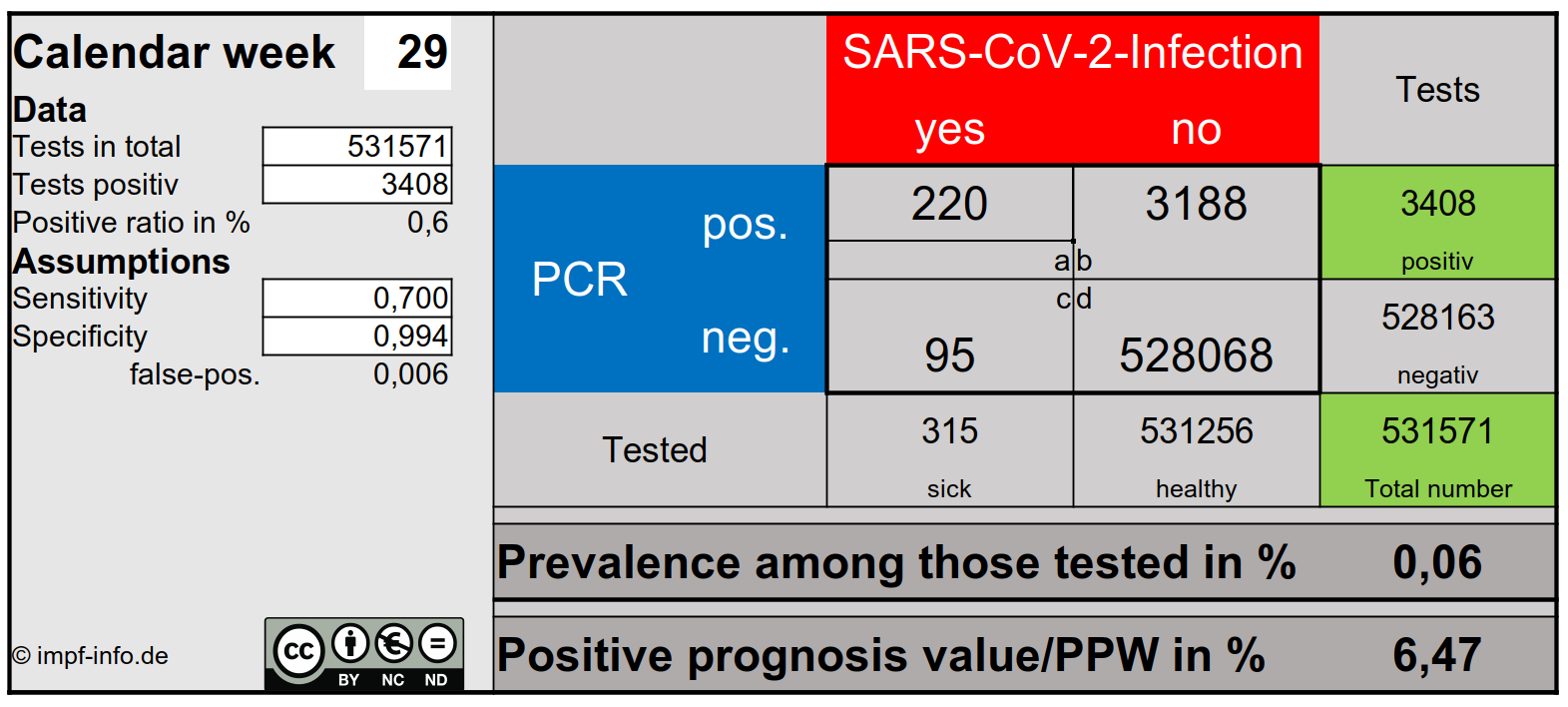
Update 15.06.2020: Here you can download a small Excel-calculator to calculate the number of false-positive test results from the RKI's figures on tests and positive test results and see how other values for sensitivity and specificity affect these figures. You can then also see (via the PPW) how low the significance of a positive test result is at present.
And here - from minute 13:10 - you can see that the (very obviously difficult) topic has meanwhile even reached the Federal Ministry of Health:

Update 12.06.2020: Applying the considerations on PCR tests listed below to the test numbers currently reported by the RKI results in the following picture:
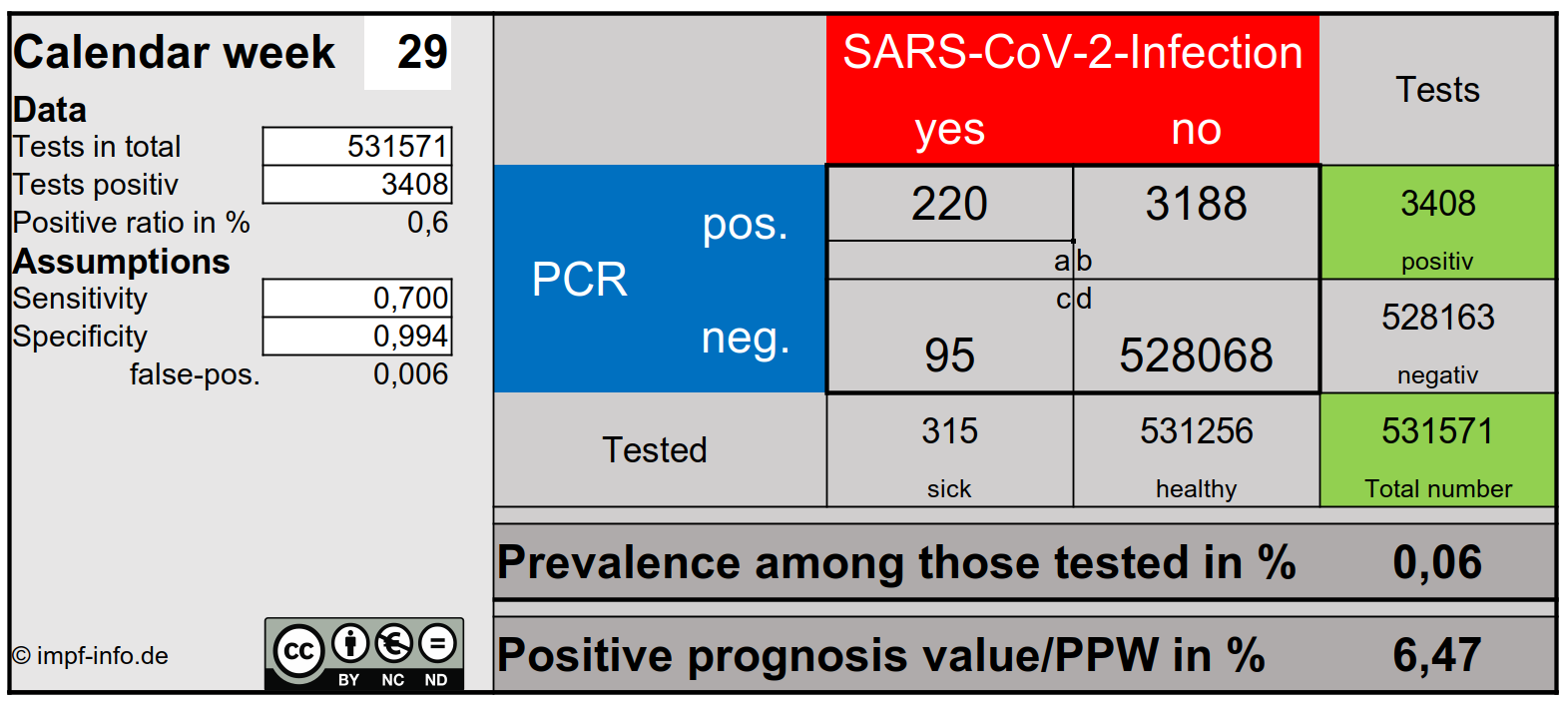
This calculation (which, for methodological reasons, only indicates orders of magnitude) is based on the following assumptions:
- An average specificity of the tests of 99.3% (Zeichhardt 2020)
- An average sensitivity of the test of 70% (Kucirka 2020 - this work finds during the symptomatic phase of COVID-19 (and in this phase is tested in Germany) sensitivities of PCR tests of 60-80%)
Interesting aspects of the calculation are (KW 24):
- With 330,000 performed tests of suspected cases of COVID-19 (i.e. a pre-selected population group) only about 1 of 300 tested persons was actually ill. This would correspond to a prevalence in this group (!) of about 0.31%.
- It can definitely be assumed that this rate is significantly lower in the normal population.
- The overwhelming majority of positive test results are false-positive, i.e. they are found in people who are actually healthy.
- Under these assumptions, a positive predictive value of only 24% results - i.e. the probability that a test result that is positively collected in week 23 actually still indicates COVID-19 disease is less than 25%, the probability that it is a false positive result is over 75%.
- This value, too, is - since the absolute number of false-positive tests is included in its calculation - strongly dependent on the number of tests: the higher the number of tests (with the same proportion of positive results), the lower the significance of the positive result/ PPV.
If you use a test to search for a disease or pathogen in a population, there are two goals:
- The test should reliably find all those who are really ill/infected, i.e. not to overlook anyone - this is called the sensitivity of a test.
- The test should reliably find only those who are really ill, i.e. who are not positive in anyone who is not ill/infected - this is called the specificity of a test.
The sensitivity and specificity of a test are its characteristics and are usually documented and published (at least to a professional audience) as part of the regulatory approval process.
All test procedures suffer from two dilemmas:
- No test is perfect - the values for sensitivity and/or specificity are never 100%, that is: - each test overlooks a part of the really ill/infected people, i.e. it shows negative test results in people where these should have been positive ("false negative results" the sensitivity is always < 100%) - each test shows positive test results in people where these should have been negative because these people are not ill/infected ("false positive results" - the specificity is always < 100%)
- Sensitivity and specificity are in a tense relationship to each other - the more sensitive a test is, the lower its specificity is usually, and vice versa.
A decisive question in testing is of course how reliably a positive test result actually indicates the presence of a disease - this is described by the so-called positive predictive value/PPV. A PPV of 100% would mean that all those who tested positive are actually ill - the further the value is below 100%, the greater the probability that a positive test is false positive.
All three values: sensitivity, specificity or the PPV are either given in % or as part of 1 - a PPV of 24% can therefore also be expressed as a PPV of 0.24, for example].
This also applies to such highly specialized tests as the so-called RT-PCR swab tests, millions of which (not only) have been performed in Germany for months and whose results - nicely colorfully packaged in lines, columns or pies - have been wrongly sold to us for months as a number of "new infections" and have been used as the basis for unprecedented restrictions of basic rights.
According to papers distributed by the RKI (Zeichhardt 2020), the SARS-CoV-2-PCR tests have - and this is where it gets exciting - a specificity of at best 99.3% (average value - which in itself is not bad!) - but this means no more and no less than that at least 0.7% of the test results are false positive.
What does that mean?
It means that if 100,000 tests are performed on safely healthy, non-infected persons, 700 of these tests are (falsely) positive - in other words, they "prove" the presence of a disease that does not (no longer) exist in this frequency.
Now, in the last documented 20th calendar week, only 1.7% of the tests in Germany are positive anyway - i.e. 1700 of 100,000.
If I subtract the 700 that are false positive from this number, the remaining 1000 - or 1%.
It is also important to keep in mind that these 1.7% positive test results in no way mean that 1.7% of the tested persons tested were positive - "It should be noted that the number of tests does not equal the number of tested persons, as the figures may include multiple tests of patients. (RKI 20.05.2020); on the one hand, this means that the recommended swabs of the nose and throat are partly (in contrast to the recommended) carried out with separate tests (then makes two tests for one tested person) and partly also control tests during the course of a disease - the systematic control of positive test results is not provided by the RKI (see below).
What else does that mean?
It means that as long as we do PCR testing on this scale, there will always be enough false-positive results to make the pandemic immortal - there are still enough "new infections"... second wave and all...
And what does that also mean?
It means that the number of supposedly "new infections found" in the late phase of the pandemic (i.e. now when there are almost no more "true new infections") depends practically only on the number of tests performed.
This in turn means that the number of positive results can be controlled by the number of tests performed: in district XY, demonstrations are to be banned again and the limit is 50 new infections/100,000 inhabitants? No problem: with 7200 tests/100,000 inhabitants the desired result is guaranteed... .
Against this background, the demand for "more and more tests", repeated like a prayer wheel by politicians, gets a completely new connotation...
And how can the problem be solved?
The simplest solution to the problem of false positive test results would be to consistently test every single person tested with a positive result immediately a second time - this is routinely done in Swiss laboratories, for example (NZZ dated 14.05.2020).
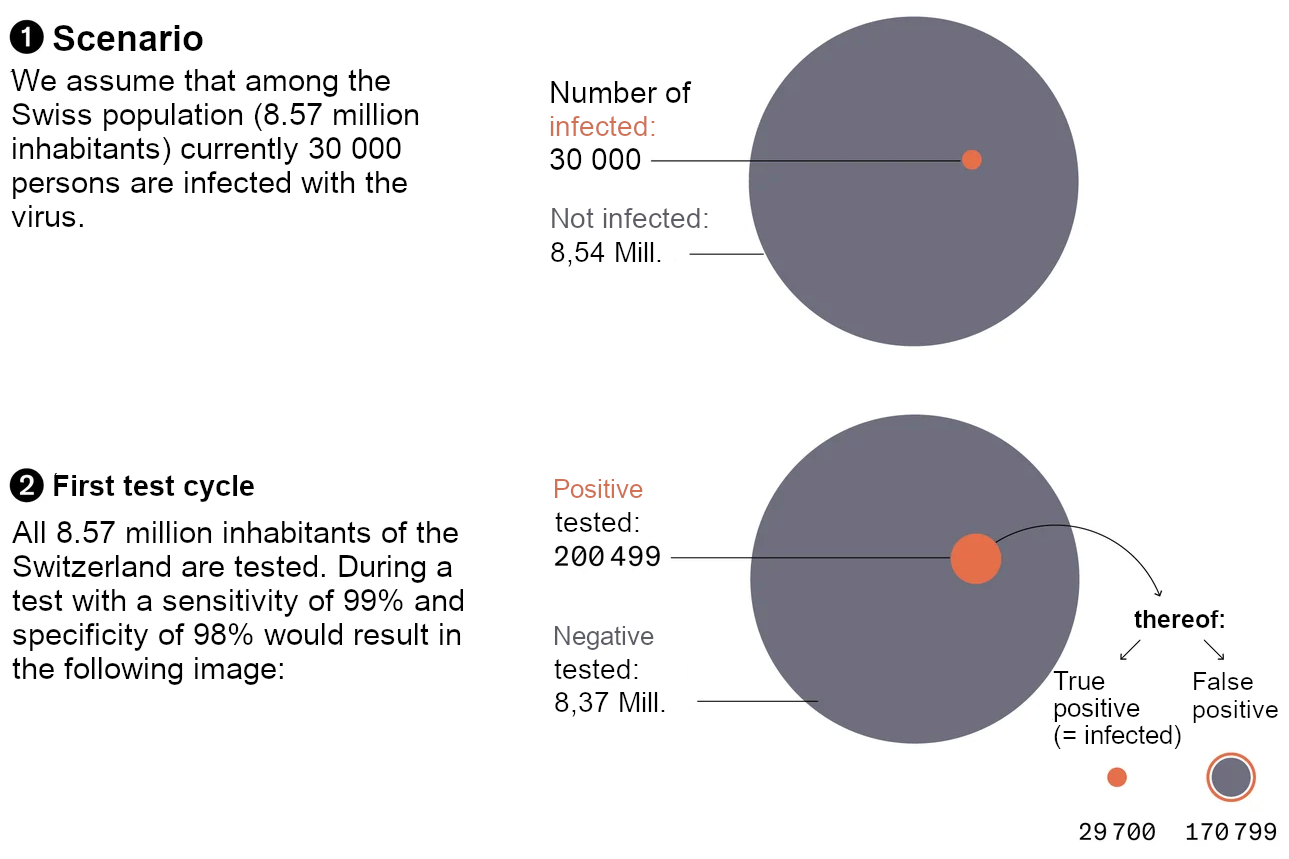
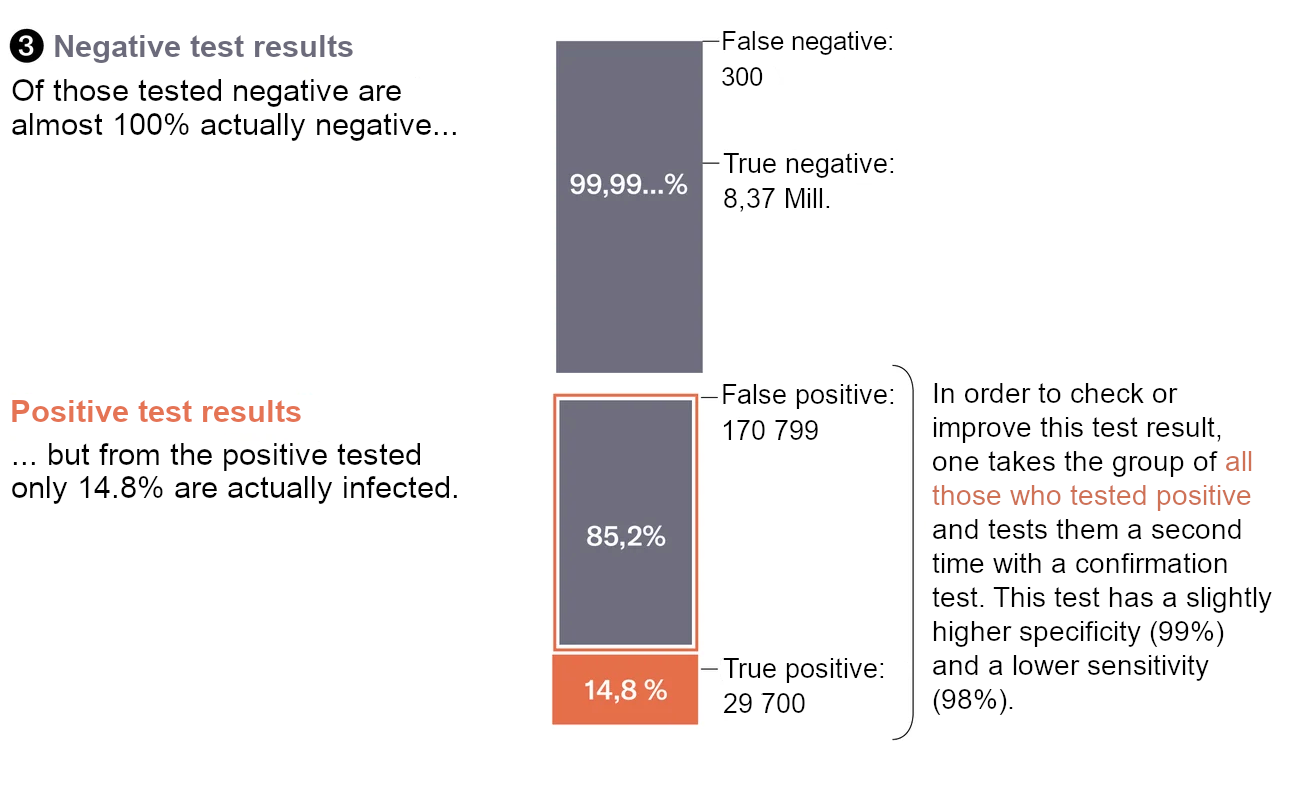
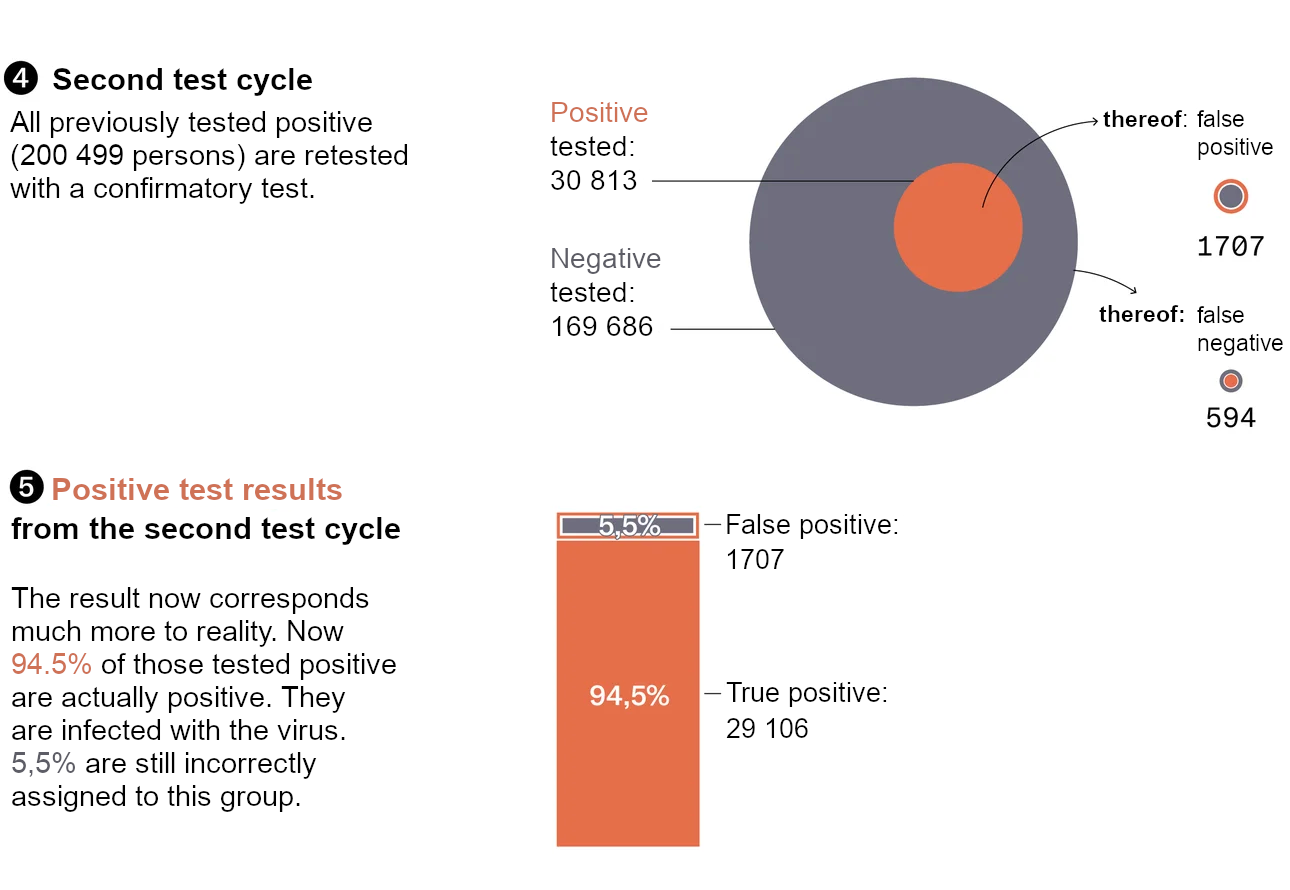
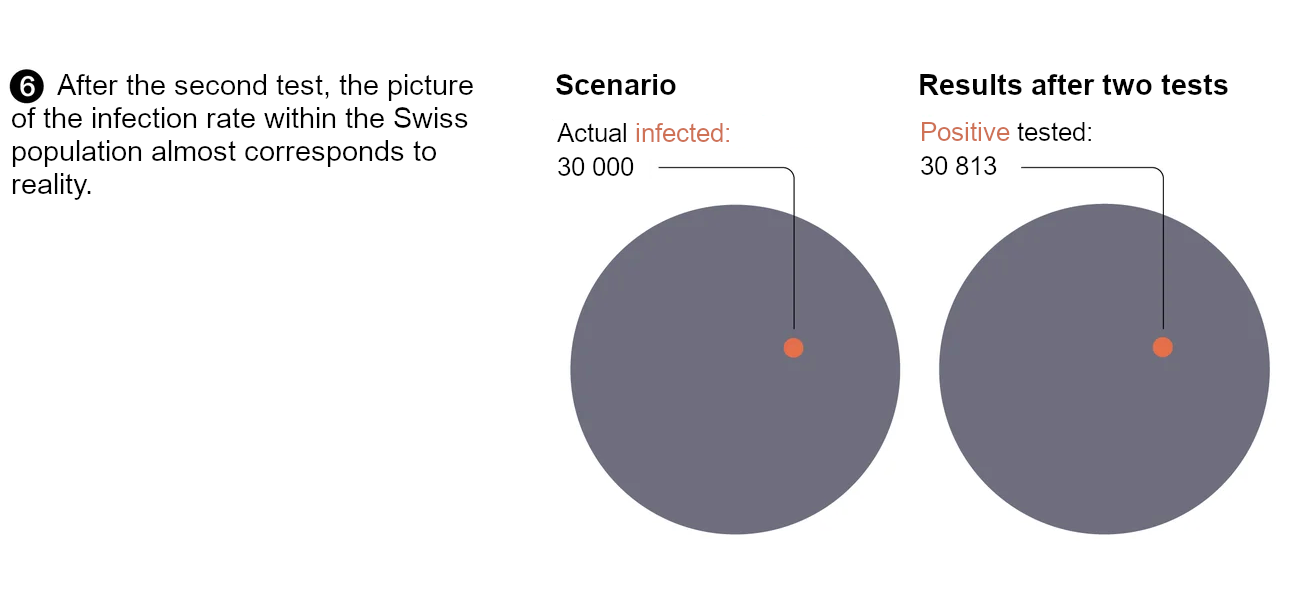
(Source: NZZ of 14.05.2020)
One waits in vain for a corresponding recommendation from the RKI.....
Test result calculator shown in this page can be downloaded from here.
Translated & reblogged Version - Original here
Telegraph main page with overview of all articles: Link
Visit our Telegram Channel for additional news & information: Link
Chat with like-minded in our Telegram Chat Group: Link
Please support to keep this blog alive: paypal