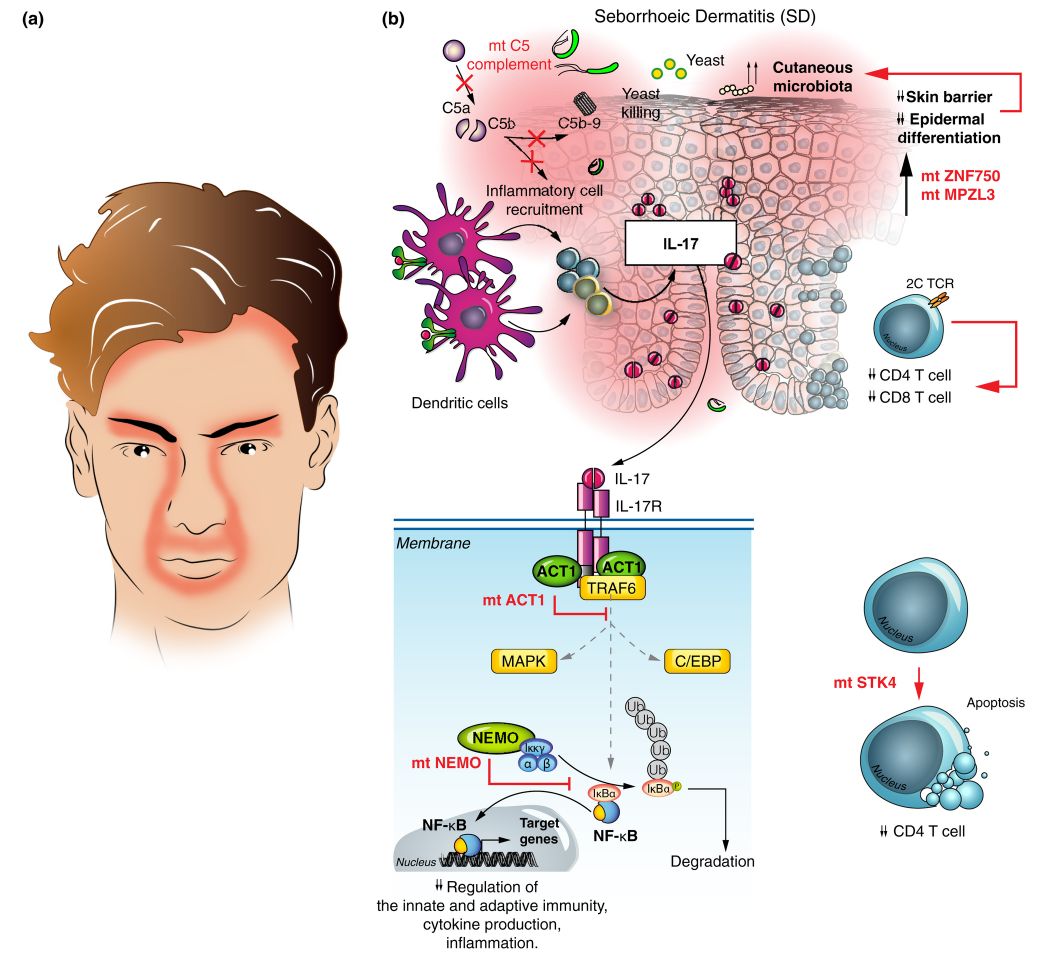
Seborrheic dermatitis
@differential_diagnosis1Seborrheic dermatitis is a chronic, relapsing, and usually mild form of dermatitis that occurs in infants and in adults. The severity may vary from minimal, asymptomatic scaliness of the scalp (dandruff) to more widespread involvement. Affected individuals are usually healthy, although seborrheic dermatitis has been associated with human immunodeficiency virus (HIV) infection, Parkinson disease, a number of other neurologic disorders, and use of neuroleptic medications.
Clinical Presentation
Seborrheic dermatitis may first appear soon after puberty or later in life. It is usually characterized by well-demarcated, erythematous plaques with greasy-looking, yellowish scales distributed on areas rich in sebaceous glands, such as the scalp, the external ear, the center of the face, the upper part of the trunk, and the intertriginous areas

Scalp
The mildest and most common form of scalp seborrheic dermatitis is dandruff, also known as pityriasis sicca, in which the scalp shows fine, white, diffuse scaliness without underlying erythema
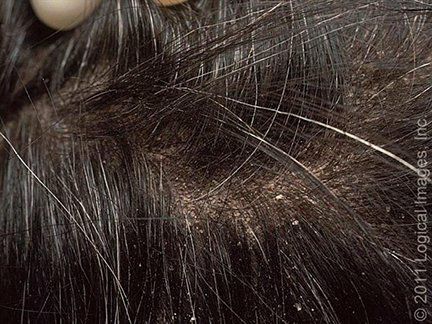
Dandruff may be asymptomatic or accompanied by mild pruritus. More severe forms of scalp seborrheic dermatitis present with visible inflammation, consisting of patchy, orange to salmon-colored or grayish plaques covered with yellowish, greasy scales (pityriasis steatoides), mostly over the temporoparietal areas

or with concretions of scale around hair shafts (pityriasis amiantacea)

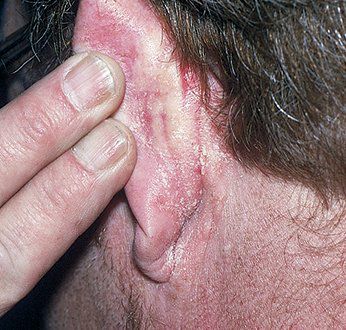
Lesions may extend to the postauricular areas, where they often develop fissures, oozing, and crusting, and to the outer canal and concha of the ear, sometimes with marked pruritus and superinfection (otitis externa).
Face
Facial lesions favor the forehead below the hairline, the eyebrows and glabella and the nasolabial folds

They may extend to the cheeks and malar areas in a butterfly distribution. The mustache and beard area are frequently involved in men with facial hair. Shaving helps with treatment and control of the disease.
Periocular
Blepharitis with redness of the free margin of the eyelids and yellow crusting between the eyelashes may be the sole manifestation of seborrheic dermatitis or may accompany its more classic distribution.
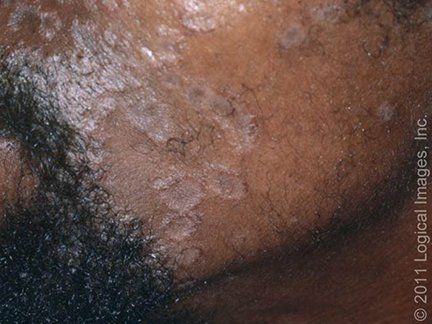
Trunk
Five patterns of truncal involvement have been described:
● Moist, erythematous intertrigo of the axillae, inframammary folds, umbilicus, and genitocrural area

● The "petaloid pattern," consisting of polycyclic, finely scaly, thin plaques over the sternum or interscapular area
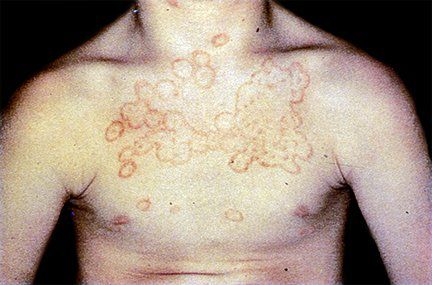
● Annular or arcuate, round to oval, slightly scaly plaques on the trunk, sometimes with hypopigmented central clearing, known as "seborrheic eczematids"
● The pityriasiform pattern mimicking pityriasis rosea, comprised of 5 to 15 mm, oval-shaped, scaly lesions distributed along the skin tension lines
● The psoriasiform pattern with larger red, rounded plaques, covered with thicker scales
Differential diagnosis
🔹️Psoriasis – Psoriasis is the main condition in the differential diagnosis of seborrheic dermatitis in adolescents and adults. Sometimes the two diseases may coexist, and the term "sebopsoriasis" has been given to those cases where the distinction cannot be made. Usually, however, psoriatic lesions are sharply demarcated and erythematous, and the scales are more abundant and silvery white. In most cases the extensor areas such as the elbows and knees are involved, although the lesions can occur in the body folds (inverse psoriasis). Characteristic nail changes, as well as the presence of arthritis or a positive family history may help establish the diagnosis of psoriasis.

🔹️Rosacea – Rosacea is another condition that commonly targets the face and sometimes coexists with seborrheic dermatitis. In contrast with seborrheic dermatitis, rosacea shows a predominance of telangiectasias and papulopustules, with frequent involvement of the nose, malar, and perioral areas and minimal or no scaliness.

🔹️Allergic contact dermatitis – Allergic contact dermatitis may be suspected in patients with seborrheic dermatitis that does not respond to standard therapy, especially if pruritus is the predominant symptom. Allergic contact dermatitis may occur concurrently or be a complication of seborrheic dermatitis in patients allergic to components of topical medications for seborrheic dermatitis or regular skin and hair care products. Patch testing may be necessary to confirm the diagnosis.
🔹️Tinea versicolor – On the trunk, petaloid lesions of seborrheic dermatitis may be mistaken for tinea versicolor, which usually lacks erythema

🔹️Pityriasis rosea – Pityriasis rosea is distinguished from seborrheic dermatitis by its abrupt onset, presence of a herald patch, and resolution within a few weeks. The pityriasiform variant of seborrheic dermatitis should be suspected when lesions appear more progressively, persist for more than three months, and are accompanied by lesions on areas usually spared by pityriasis rosea (the face and intertriginous areas).

🔹️Tinea corporis – Annular or arciform seborrheic dermatitis lesions on the trunk can be confused with tinea corporis; tinea corporis can be ruled out by negative potassium hydroxide (KOH) microscopic examination and negative fungal culture.
🔹️Secondary syphilis – Secondary syphilis, the great imitator, can trigger widespread pityriasiform or psoriasiform eruptions that can be mistaken for seborrheic dermatitis. Additional signs such as palmoplantar and mucosal lesions or peripheral adenopathy should be looked for, and appropriate serologic testing ordered when indicated.
🔹️Lupus erythematosus – Seborrheic dermatitis of the face may be mistaken for the butterfly eruption of acute systemic lupus erythematosus (SLE) or the discoid plaques of cutaneous LE. The acute eruption of SLE rarely involves the nasolabial sulcus or crosses the bridge of the nose. Discoid lesions exhibit atrophy and sometimes scarring, along with adherent scales that may have "carpet tacking" on their undersurface (spiny projections that plug dilated follicular openings). Histologic examination and serologic testing for antinuclear autoantibodies should be performed to confirm the diagnosis.

🔹️Pemphigus foliaceous – Pemphigus foliaceous is characterized by erythema, scaling, painful erosions, and crusting that first appear on the face and scalp and later involves the chest and back. Histology, direct immunofluorescence, and the measurement of circulating autoantibodies against desmoglein establish the diagnosis. Pemphigus erythematosus of Senear and Usher is a superficial variant of pemphigus foliaceous that is most likely to mimic seborrheic dermatitis.


✏ Prescription sample (نسخه) 👇👇
📌 Related posts
1.Differential diagnosis of Psoriasis