Pulmonary Embolism In Pregnant Women
🛑 👉🏻👉🏻👉🏻 INFORMATION AVAILABLE CLICK HERE👈🏻👈🏻👈🏻
РекламаGianFranco Ferre For Women - Производство Италия - Бесплатная доставка от 2 000р.
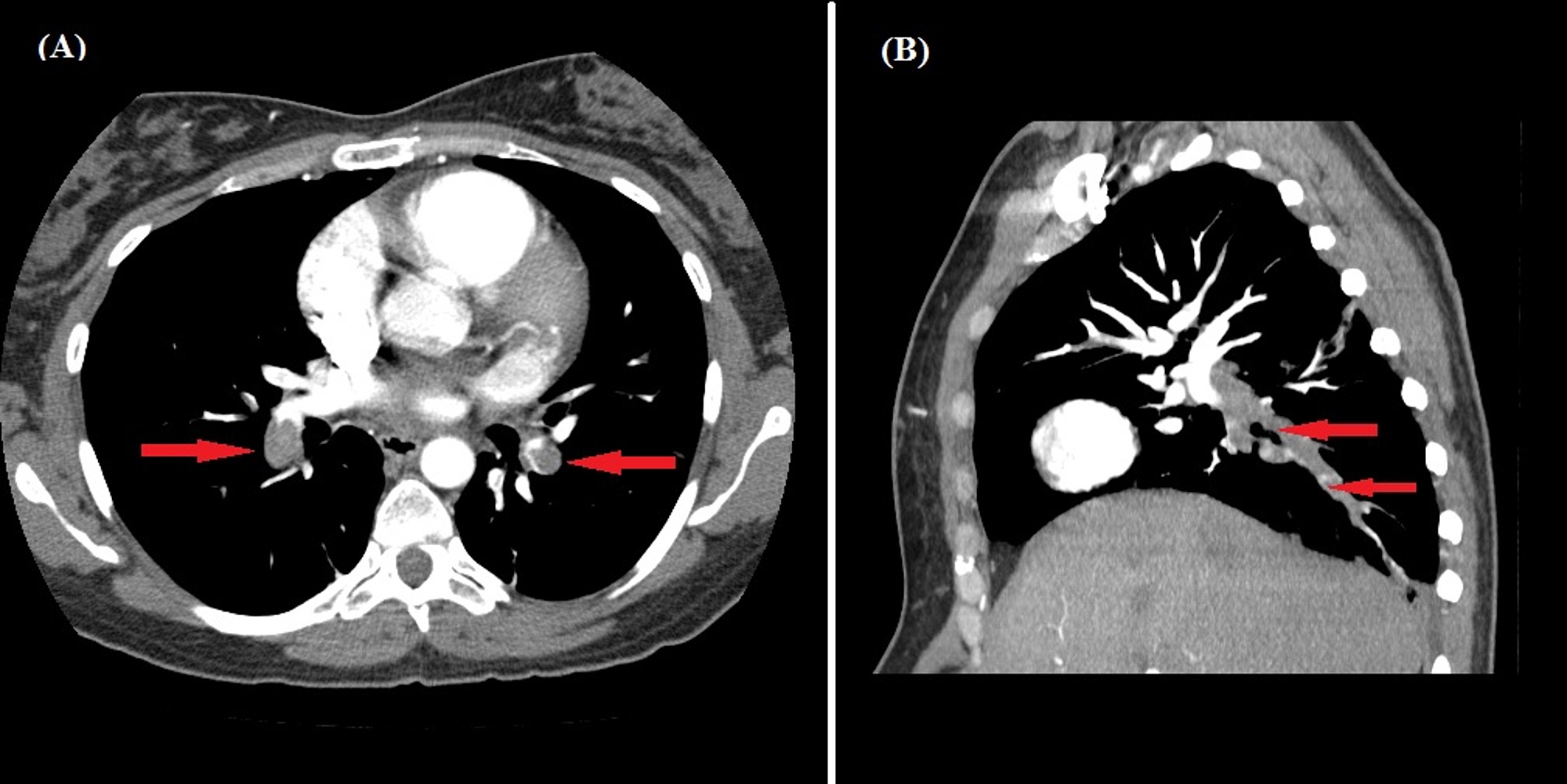
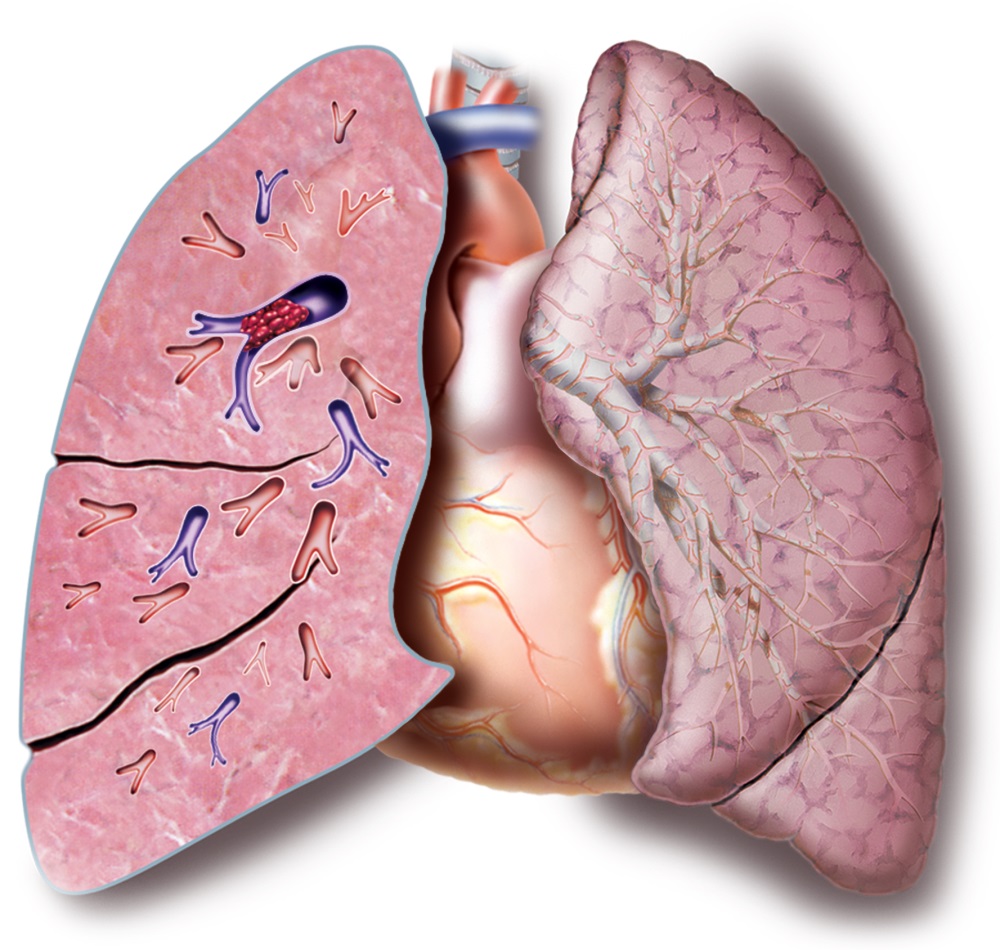
Pulmonary embolism during pregnancy is the most dreaded medical condition. It is one of the most prominent causes of maternal mortality in developed countries. Pulmonary embolism is defined as obstruction of pulmonary artery in the lung. Blockage mainly results from a blood clot that migrates from a site outside the lungs in a pregnant woman.
Who is more at risk for pulmonary embolism during pregnancy?
Who is more at risk for pulmonary embolism during pregnancy?
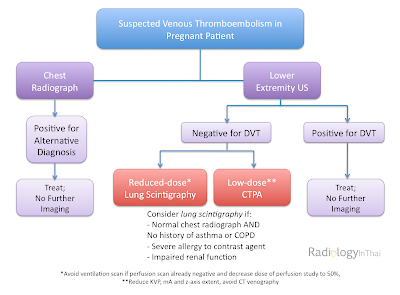
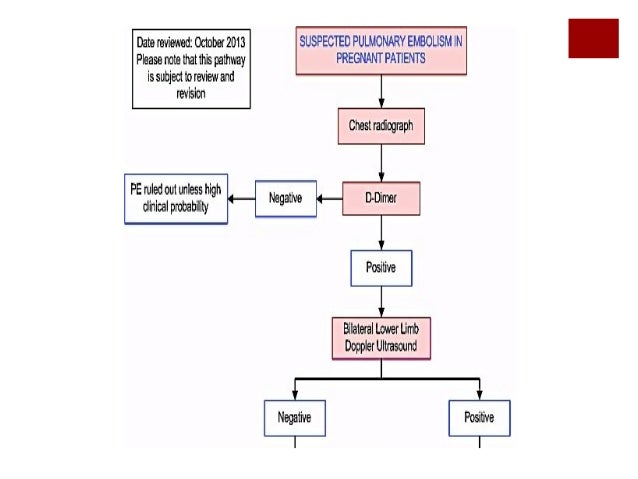
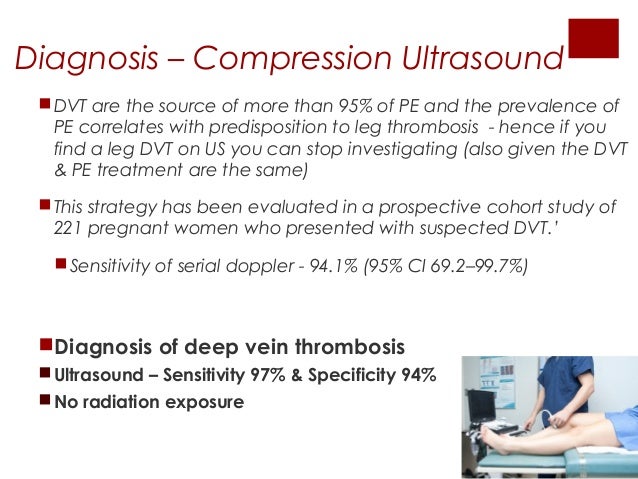
Pregnant and postpartum women are two to four times as likely as nonpregnant patients have venous thromboembolism [ 1 – 3 ]. Deep venous thrombosis (DVT) is more common than PE, and postpartum women are at higher risk than pregnant women [ 4 ]. Ultrasound is well-established as the technique of choice for diagnosing DVT.
www.ajronline.org/doi/full/10.2214/AJR.09.3…
Can a perfusion scan detect pulmonary embolism in pregnancy?
Can a perfusion scan detect pulmonary embolism in pregnancy?
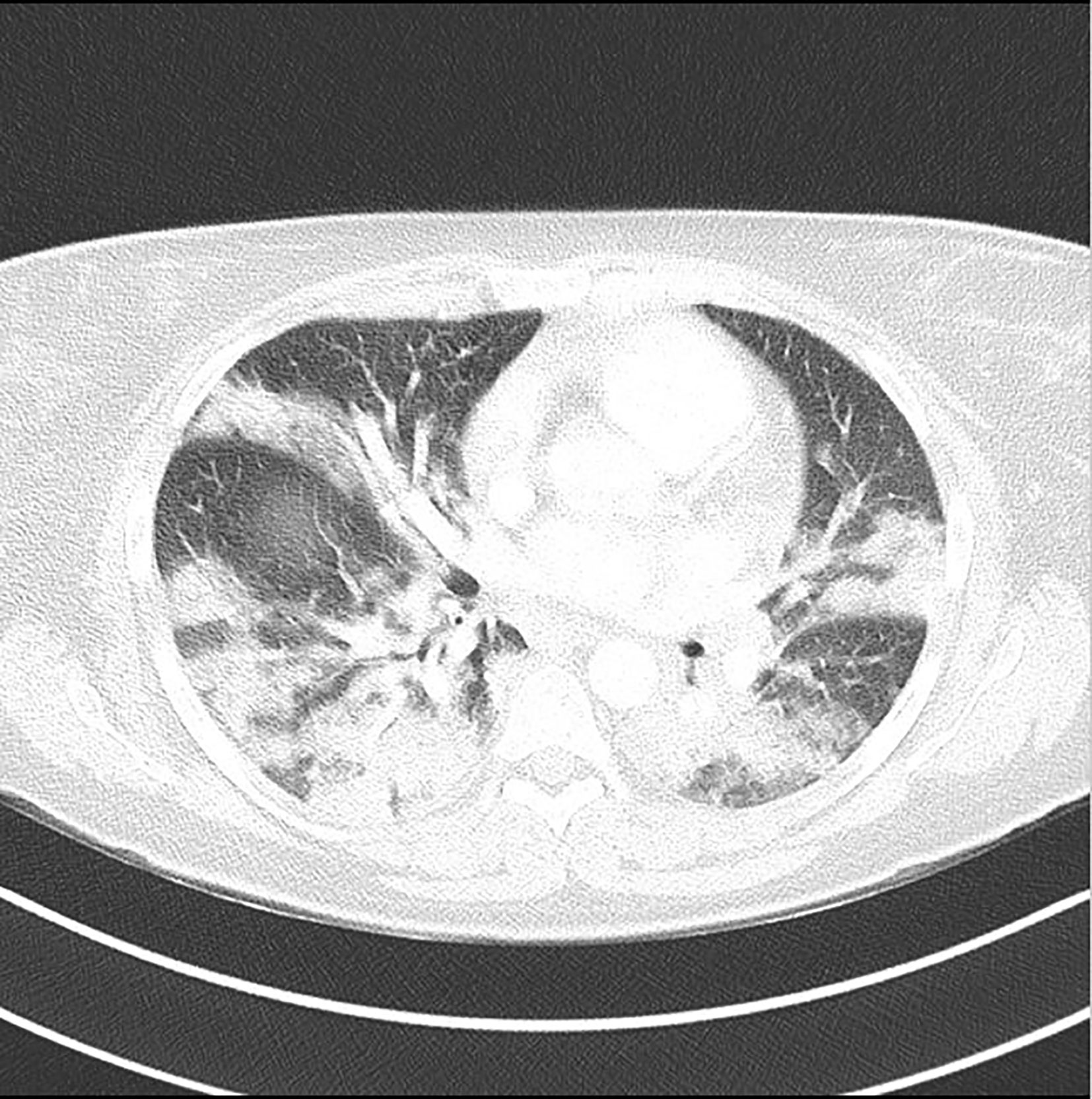
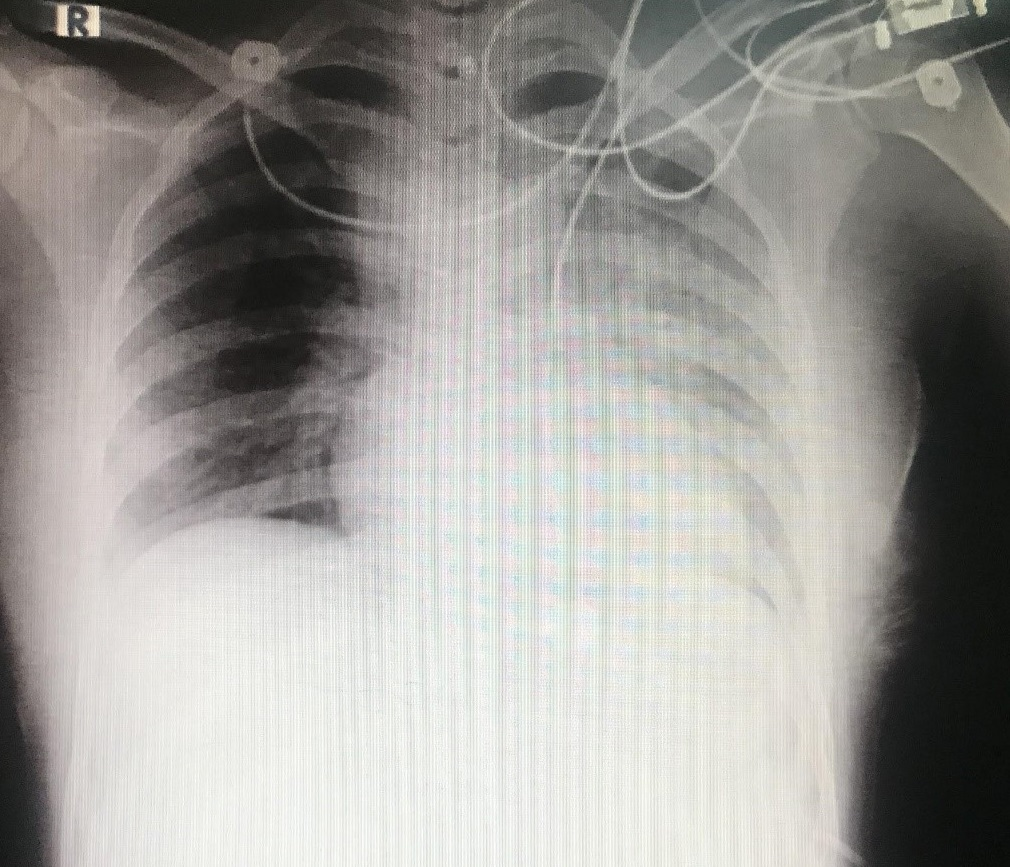
Both CT pulmonary angiography and perfusion scanning are well-established techniques for evaluating PE. The number of imaging studies for venous thromboembolism during pregnancy has increased dramatically [ 5 ]. At one university hospital, such imaging has increased more than fivefold.
www.ajronline.org/doi/full/10.2214/AJR.09.3…
What are the symptoms of a pulmonary embolism?
What are the symptoms of a pulmonary embolism?
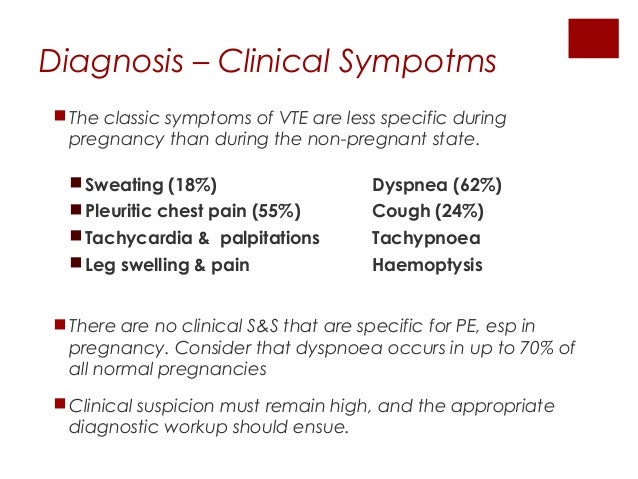
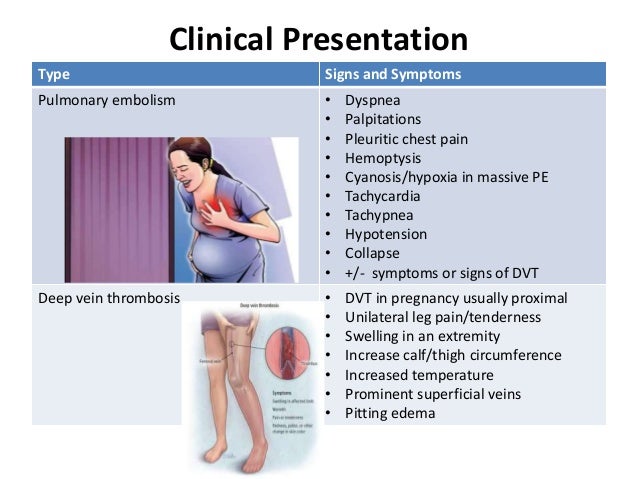
The most common symptoms — shortness of breath, chest pain, and leg swelling — are also general pregnancy symptoms, which makes it difficult to discern if the symptom is the result of a PE or not. To diagnose PE, obstetricians rely heavily upon patient history and general health to assess whether or not a patient has a suspected embolism.
weillcornell.org/news/what-every-woman-s…
Why did ROA have a pulmonary embolism during pregnancy?
Why did ROA have a pulmonary embolism during pregnancy?
Nurses clocked her heart rate at 220 beats per minute. It took two days and a barrage of tests for doctors to discover the cause of her symptoms: a pulmonary embolism . A large blood clot in Roa’s lungs was blocking her breathing and stressing the right side of her heart.
www.yalemedicine.org/news/pulmonary-em…
https://pubmed.ncbi.nlm.nih.gov/33548928
Thrombolysis or embolectomy should be considered for pregnant women with pulmonary embolism complicated by hemodynamic instability. Treatment of pregnancy-associated pulmonary embolism …
https://www.yalemedicine.org/news/pulmonary-embolism-pregnancy
11.10.2017 · Pulmonary emboli can have a high fatality rate when a patient has very low blood pressure or an overly slow heart rate. “In a patient at term pregnancy, our treatment options are extremely limited, and both the patient’s and baby’s life are in peril,” says Yale Medicine’s Leon Freudzon, MD, an assistant professor in anesthesiology at Yale School of Medicine, who was part of the team helping Roa.
Тромбоэмболи́я лёгочной арте́рии — закупорка лёгочной артерии или её ветвей тромбами, которые …
eMedicine: med/1958 emerg/490 radio/582
Текст из Википедии, лицензия CC-BY-SA
https://pubmed.ncbi.nlm.nih.gov/32371163
Pulmonary embolism in a young pregnant woman with COVID-19. Pulmonary embolism in a young pregnant woman with COVID-19. Pulmonary embolism in a young pregnant woman with COVID-19. Pulmonary embolism in a young pregnant woman …
https://weillcornell.org/news/what-every-woman-should-know-about-pregnancy-and...
24.04.2017 · It is difficult to detect PE in pregnant women because the circulatory system changes considerably throughout pregnancy. The most common symptoms — shortness of breath, chest pain, and leg swelling — are also general pregnancy symptoms, …
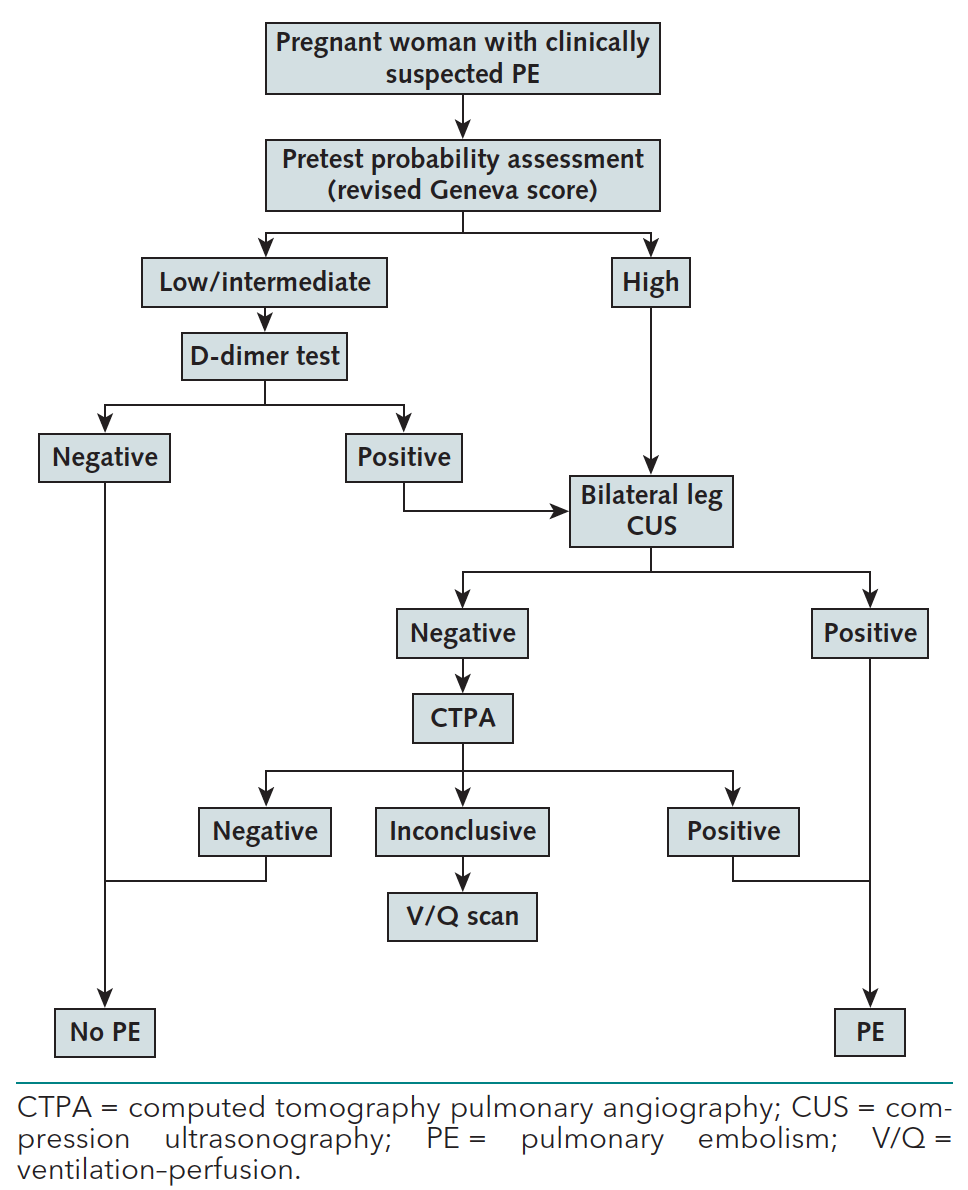
Pregnancy Adapted YEARS Algorithm for Diagnosis of Suspected Pulmonary Embolism
Coronavirus survivor talks about being first to have double lung transplant
Husband of pregnant woman on life support sues hospital
DVT/Pulmonary Embolism (old version, with sound) - CRASH! Medical Review Series
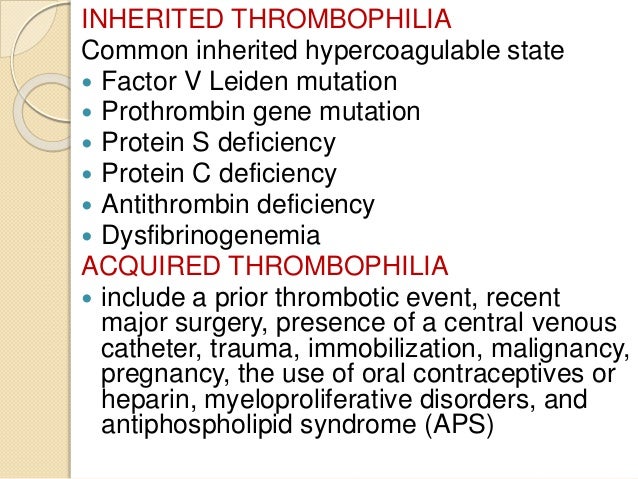
VENOUS THROMBOEMBOLISM IN PREGNANCY
https://aci.health.nsw.gov.au/.../eci/clinical/clinical-tools/respiratory/pe/pe-pregnant
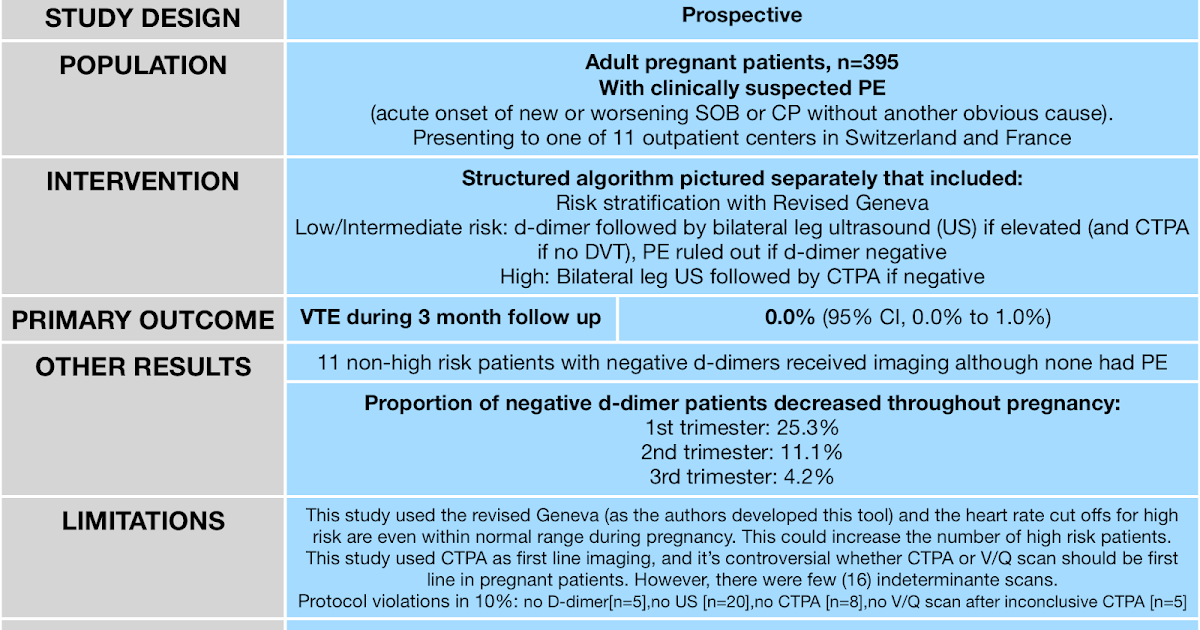
03.12.2020 · The risk of pulmonary embolus in the non-pregnant female risk is 1 in 100,000 increases to 1 in 10,000 in pregnant age-matched females. From Kline’s own work, 60% of healthy patients in normal pregnancy will have a raised D-dimer. He proposes using the PERC rule, adapted for normal physiological change in heat rate during pregnancy, in combination with an altered D-dimer threshold to risk stratify pregnant …
https://www.ajronline.org/doi/full/10.2214/AJR.09.3506
Pulmonary embolism (PE) is a potentially fatal disease during pregnancy. Pregnant and postpartum women are two to four times as likely as nonpregnant patients have venous thromboembolism [ 1 – 3 ]. Deep venous thrombosis (DVT) is more common than PE, and postpartum women are at higher risk than pregnant women …
https://www.tandurust.com/pregnancychildbirth/pulmonary-embolism-in-pregnancy.html
01.12.2015 · Pulmonary embolism in pregnant women mainly develops due to deep vein thrombosis in the leg. Together with the symptoms of pulmonary embolism, patient may also have symptoms of deep vein thrombosis. The symptoms of pulmonary embolism …
РекламаGianFranco Ferre For Women - Производство Италия - Бесплатная доставка от 2 000р.
Александровск-Сахалинский, Сахалинская область
Александровск-Сахалинский, Сахалинская область
Не удается получить доступ к вашему текущему расположению. Для получения лучших результатов предоставьте Bing доступ к данным о расположении или введите расположение.
Не удается получить доступ к расположению вашего устройства. Для получения лучших результатов введите расположение.
With the help of a team of Yale Medicine experts, a near-death experience results in new life for a young family.
Late at night on Feb. 11, 2015, an ambulance raced up I-95 toward Yale New Haven Hospital.
The day before, Victoria Roa, 38 weeks pregnant, had felt dizzy when she went to lift her young son, Nicholas, out of his crib. Her chest hurt, and she struggled to breathe. She called to her fiancé for help, and then telephoned her obstetrician. He told the 33-year-old resident of Harrison, N.Y., to go straight to the emergency room.
“I told them to save my son, without a doubt. I’d lived. He hadn’t lived yet. I wanted him to get a chance at life. I didn’t want him to die.”
Roa went to Greenwich Hospital, where she had planned to deliver her baby. Nurses clocked her heart rate at 220 beats per minute. It took two days and a barrage of tests for doctors to discover the cause of her symptoms: a pulmonary embolism. A large blood clot in Roa’s lungs was blocking her breathing and stressing the right side of her heart. Her life was in immediate danger.
“They said they couldn’t handle the situation there, they were going to rush her to Yale,” says Roa’s younger sister, Maria Lagani.
When Roa’s ambulance reached the hospital, a team of doctors and nurses from Yale Medicine ran out to meet it. As they admitted her and started planning her treatment, they asked her a painfully difficult question. “If they could only save one life—mine or my baby’s—which did I want them to save?” Roa says.
Pulmonary emboli can have a high fatality rate when a patient has very low blood pressure or an overly slow heart rate. “In a patient at term pregnancy, our treatment options are extremely limited, and both the patient’s and baby’s life are in peril,” says Yale Medicine’s Leon Freudzon, MD, an assistant professor in anesthesiology at Yale School of Medicine, who was part of the team helping Roa.
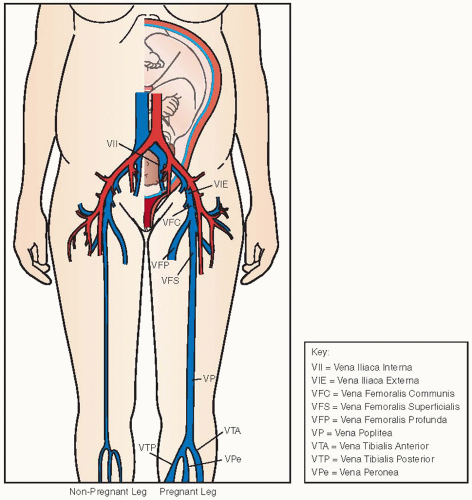
Roa’s clot had probably started in a vein in her leg. This is not uncommon in pregnant women, because the uterus can obstruct blood flow to the lower extremities, leading to what is called a deep vein thrombosis. Roa’s baby had been putting pressure on her right hip, and she had had to leave her job as a massage therapist before her planned maternity leave. She had been using crutches to get around. Her limited mobility may have contributed to the formation of the clot.
“Occasionally, the clots can travel up to the heart and lungs,” says Pramod Bonde, MD, a Yale Medicine cardiac surgeon and an associate professor of surgery at Yale School of Medicine, who also cared for Roa. “They reduce the amount of blood going to the left side of the heart, and put a lot of stress on the right side.”
When Roa arrived at Yale, her heart was struggling against the clot. Her life, and that of her baby, hung in the balance.
Still, Roa did not hesitate when answering the caregivers’ question. “I told them to save my son, without a doubt,” she says. “I’d lived. He hadn’t lived yet. I wanted him to get a chance at life. I didn’t want him to die.” But Roa’s mother, Deborah Tarasoff, objected, equally protective of her daughter’s life. She insisted that they call Roa’s fiancé, Gerald, who was at home with the couple’s other child. The two begged her to change her mind. “They both said, ‘Without you, it will be hard for the baby to survive,’” she says. “We have to save you.” She finally acquiesced.
A multidisciplinary team assembled for a meeting. The physicians included a maternal-fetal specialist, Katherine Kohari, MD; the heart surgeon, Dr. Bonde; the cardiac anesthesiologist, Dr. Freudzon; and Ferne Braveman, MD, director of the Department of Obstetrics & Gynecology Anesthesiology. “We discussed the case at length to figure out the safest thing to do,” Dr. Freudzon says.
“There were no egos,” Dr. Braveman says. “The entire team of physicians and nurses was focused on doing the best thing for the mom and the baby. Because we didn’t have one patient, we had two.”
The team’s main concern was that Roa’s heart could stop at any moment. The usual medical response to a stopped heart is CPR. “It doesn’t work as well for a pregnant woman,” Dr. Freudzon says. “Because you have a baby in there, it prevents the return of the blood to her heart. CPR would not rescue her.” If Roa’s heart stopped, she and the baby could die.
Another worry was that Roa would go into labor, further stressing her heart and making it difficult for the team to mobilize for cardiac anesthesia and heart surgery.
Also a problem: Roa was taking blood thinners to keep the clot from growing. Those medications could cause excessive bleeding if the Yale Medicine team performed a cesarean section (C-section). “We were between a rock and a hard place,” Dr. Braveman says.
They had a few tough options, says Dr. Bonde. One was to do what would be typical for most hospitals: Watch and wait to intervene. If the heart failed, a surgeon would crack open the patient’s chest to deal with the clot and the stopped heart. With this approach, “The expected mortality for the mother and the baby would be very high,” Dr. Bonde says. Another possible choice was to attempt to extract the clot through surgery, but the expected outcome of that procedure was not much more hopeful.
Eventually, Roa’s extremely precarious position forced an action. “We didn’t know how much strain the right side of her heart could take,” Dr. Freudzon says.
Dr. Bonde said that they would have the best chance for a healthy baby and healthy mother if they did a C-section, but one performed in a way to save Roa’s life in case her heart stopped. “We decided that instead of CPR, we’d do cardiopulmonary bypass,” Dr. Freudzon says.
It had to be carefully planned. Before doctors started the C-section, they would place catheters in blood vessels in Roa’s groin. If her heart stopped during the surgery, her blood could immediately be diverted to a machine that would oxygenate it and return it to her body.
This approach required Dr. Bonde to use his specialized training and advanced equipment to suction out the clot through the catheters. “We could save both the mother and the baby, without doing any harm to them,” he says.
Everyone in the operating room was ready to step in if their skills were needed. “They told us how they planned to do everything,” Roa says. “They were going to try to save the baby, too. We thought, ‘We’ll see how it goes down.’”
The operation was done in the cardiac operating room. Regional anesthesia was not an option because of the blood thinners Roa was taking. “You can’t safely put in a spinal or epidural catheter, because you might get bleeding around the spinal cord,” Dr. Freudzon says. Instead, he administered general anesthesia. Once Roa was safely sedated, Dr. Bonde made the incisions to insert the catheters into her groin.
Meanwhile, Roa’s mother and sister huddled in the waiting room. About two hours into the procedure, a doctor hurried out with some news. “They got the baby,” he said. “Come! Come! They’re taking him to the NICU (neonatal intensive care unit).”
Tarasoff and Lagani rushed over to catch a glimpse of the family’s newest addition. “He was all wrapped up in blankets with a hat on his head,” Lagani says. “He was very out of it, because he got a lot of the general anesthesia. They had him all tubed up and were breathing for him.”
They asked, “What’s going on with Victoria?” The doctor replied: “They’re working on her now. Someone will come out and talk to you.”
A torturous hour and a half ticked by before another doctor came out to speak with the two women. The doctors were still working on Roa, and he explained what they were doing.
Two hours later, they received a phone call from the doctor. “They said she’d been taken back to the ICU, and we should go there,” Lagani says. The women rushed over, and waited outside Roa’s room while the care team settled her in. Finally, they were allowed to come closer.
“That was one of the hardest times,” Lagani says, a sob catching in her throat. “She was yellowish, and had tubes in because a ventilator was breathing for her. She looked like the person who didn’t make it.”
Still, the Yale Medicine doctors seemed optimistic, explaining how things had gone in the operating room and what they were doing for her. They left her in the hands of the ICU nurses, who were “amazing,” Lagani says. “They were so comforting,” she says.
As one nurse attended to Roa, the ventilator buzzed, scaring her mother and sister. “That means she’s overbreathing the ventilator,” the nurse says. “That’s a good sign.”
“My mom and I were talking to her,” Lagani says. “Saying, ‘Keep breathing, keep breathing. Keep fighting.’”
Despite her life-threatening condition and the challenging surgery, Roa was doing better than anyone had dared to hope. Losing some blood during the surgery had actually improved her heart dynamics.
The doctors hoped that Roa would continue to improve after the baby’s birth, which meant her blood volume could slowly return to normal. If everything continued to go well, they could allow her body to break down the clot itself, without further medical intervention.
The day after her C-section, Roa was awake and breathing well enough to come off the ventilator. In the NICU, her baby, Joseph, had his breathing tube removed, and was taking his first gulps of air. Mother and son could finally meet.
“I started crying the moment they brought him in,” Roa says. “I was absolutely hysterical. I said: ‘Oh my God, what you put me through! I love you!’”
The two spent more time bonding the next day, Sunday, Feb. 14. “That was the best Valentine’s Day present I ever got in my life,” she says.
By the following Tuesday, Joseph was healthy enough to go home to his father and his big brother. Roa needed a few more days to convalesce and went home on Thursday. “I couldn’t believe how well I was treated at Yale,” she says. “Even after discharge, they were all calling me afterward. How was I doing? Did I have any questions? The doctors and nurses were all amazing.”
A few weeks later, Lagoni emailed Dr. Bonde photos of Joseph, on behalf of her sister. “My family and I couldn’t be more grateful for the team of doctors who saved her life,” she told him. “Thank you for all you have done!”
Mature Long Hair Porno
Twerk Compilation Solo 18
Hentai Bondage Girl
Mature Piss Face
Webcam Erotic Tv
Pulmonary Embolism in Pregnancy - PubMed
Pulmonary embolism in a young pregnant woman with COVID-19
What Every Woman Should Know About Pregnancy and Pulmonar…
Pulmonary Embolism - PE - Evaluation in the pregnant ...
Pulmonary Embolism in Pregnancy: CT Pulmonary Angi…
Pulmonary Embolism In Pregnancy: Causes, Symptoms …
Pulmonary Embolism In Pregnant Women