Provide Discomfort Administration: Meeting PUAEME008 Competency Demands
Pain control is one of those skills that specifies the top quality of frontline treatment. When a patient is wriggling on the floor of a manufacturing facility, or a youngster is panicked after a compound fracture at a weekend break game, you do not have lengthy to make audio decisions. PUAEME008, Supply Discomfort Administration, orders what proficient -responders must do to evaluate discomfort, choose and supply risk-free analgesia, display end results, and hand over treatment. It is more than a device of competency. It is a small in between a medical professional and a client in distress.
I have provided and analyzed this system for mixed groups, from remote mine paramedics to municipal occasion paramedics, and the same styles show up every program: recognize your pharmacology and contraindications, respect consent and regulation, never forget non‑pharmacological care, and file as if another person will require to run with the baton ten minutes later on. This article unboxes PUAEME008 in useful terms and provides a functioning picture of what skilled efficiency appears like in genuine environments.
Where PUAEME008 Sits in PracticePUAEME008 beings in the general public Safety And Security Educating Package and is commonly packaged into pain monitoring programs run by registered training organisations for emergency responders and allied wellness specialists working in austere or prehospital contexts. Learners are commonly already trained in key survey, air passage administration, standard life support, and scene security. The provide discomfort administration program improves that foundation to address risk-free, reliable analgesia across a spectrum of clients and environments.
Providers differ throughout Australia. Some deliver the device as a standalone pain administration certification course, others fold it right into more comprehensive programs like remote location first -responder training. For nurses and physio therapists that work in occasion medicine, occupational wellness, or remote outreach, it can enhance expert registration by formalising prehospital analgesia abilities. It is not an alternative to a tertiary discomfort fellowship. Rather, it is a concentrated emergency situation emergency pain management pain management component that asks a vital inquiry: can you alleviate discomfort rapidly and securely while expecting deterioration?

PUAEME008 assessors try to find clear, observable performance. The wording varies a little throughout variations, however the core needs continue to be stable:
Recognise and examine sharp pain utilizing structured devices suited to the client and situation. Select suitable analgesic strategies, consisting of non‑pharmacological techniques, according to protocols, scope of method, and offered resources. Administer analgesia safely using accepted routes, dosages, and tools while maintaining infection control. Monitor reaction, damaging effects, and crucial indicators, then titrate or stop therapy accordingly. Communicate plainly, gain authorization, document, and turn over to a higher level of care.These aspects sound tidy theoretically. Genuine scenes are not. You will certainly assess a client with distracting injuries and a gale blowing sand into your eyes. You will search for a radial pulse while a group films on their phones. Skills shows in just how you develop a fast but trustworthy photo, keep the individual involved and tranquility, and apply a protocol without tunnel vision.
Assessment and Triage: Checking Out Discomfort, Not Thinking ItPain is subjective and greatly coloured by worry, society, and context. A jackaroo with a disjointed shoulder might rate his pain at six yet look light and clammy with a heart price of 130. A child could reject to talk yet wince with a light touch. PUAEME008 anticipates responders to use pain scales that fit the patient. The numeric ranking scale from 0 to 10 matches articulate grownups. The Wong‑Baker faces scale helps with interaction with kids or people who like aesthetic hints. For non‑verbal people, behavioural devices such as the FLACC range assistance, though they call for method to stay clear of overcalling distress as pain.
Acute discomfort assessment in the area ought to not drift right into a long interview. Slow within the primary and secondary studies. Begin with life risks, after that a focused discomfort background: area, start, character, radiation, intensity, time course, worsening or alleviating aspects, and previous anesthetics. Pulse oximetry, heart rate, respiratory rate, blood pressure, and skin signs supply context. Note warnings that alter the strategy: altered psychological state, suspected major hemorrhage, breast pain with hemodynamic instability, severe head injury, or signs of sepsis. PUAEME008 wants -responders to acknowledge when analgesia is required and when assistance of airway, breathing, and blood circulation has to precede it by minutes that really feel much longer.
Anecdotally, one of the most common evaluation mistake from new learners is failing to reassess. They catch a standard discomfort rating, supply an opioid, after that go on with other tasks. Ten minutes later the pain has actually held one's ground, yet since no organized reassessment occurred, the opportunity to titrate is shed. Great method is easy. Tape a discomfort score before treatment, then again every 5 to 10 mins or after each dose. Combine it with vitals and an observation of sedation level, so you can discover respiratory depression early.
Pharmacological Options: What's in the Kit and When to Make use of ItThe provide discomfort management training course shows medicinal selections lined up to organisational methods. Accessibility differs. Remote centers may equip methoxyflurane, intranasal fentanyl, paracetamol, and advil. Event paramedics may operate under standing orders for dental analgesics just. Paramedic services include IV morphine, ketamine, and in some cases nitrous oxide.
Paracetamol stays the peaceful workhorse. At restorative dosages it minimizes discomfort in bone and joint injuries and soft tissue trauma. It also sets well with NSAIDs for a collaborating impact. Check for recent intake to avoid collective poisoning, specifically in smaller grownups or those with liver illness. Advil and various other NSAIDs bring anti‑inflammatory advantages however bring bleeding and renal threats. Post‑operative individuals, the senior with inadequate renal get, and people on anticoagulants may be much better served by different strategies.
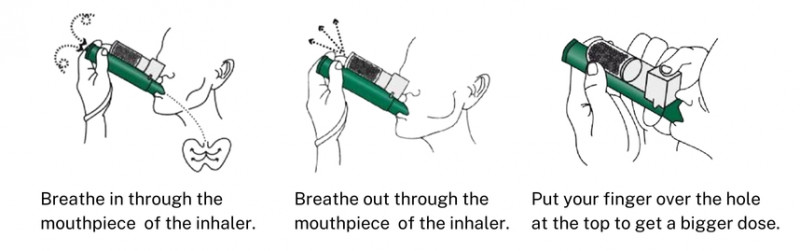
Methoxyflurane, delivered by means of a handheld inhaler, has a loyal complying with in the area. Its fast start and patient‑controlled nature fit short, uncomfortable treatments like reducing a disjointed shoulder or splinting a fracture. Look for sedation, hypotension, and the advancing dosage limitation. Several procedures top it at two 3 millilitre vials in 24 hr. I have had people who barely touched the inhaler after the first min because concentrated coaching and splinting alleviated. Others needed the full allocation to assist in extrication. It is tempting to get along with techniques while the person is calm, however if their vitals fad badly, stop and reassess before continuing.
Intranasal fentanyl bridges a vital space when IV access is not viable. Appropriate dosing based on person weight and distribution using a mucosal atomisation device yields fast analgesia. It is especially handy in paediatrics where cannulation delays treatment. Despite the convenience, treat it with the respect you would certainly any type of opioid. Know your contraindications, monitor respiration, and have naloxone ready, prepared, and around. Two percent of students fail to remember to prime the atomiser during simulations, which lowers effectiveness. Build a behavior of a fast equipment list before administration.
IV opioids continue to be staples for many solutions. Titrated increments of morphine or fentanyl allow accurate control. I prefer tiny boluses tied to duplicated pain ratings and sedation analyses instead of large front‑loaded doses, particularly for older grownups. Ketamine offers a dissociative course for severe discomfort, especially in injury where hypotension looms. Reduced dose ketamine for analgesia varies from induction doses used in step-by-step sedation. Nystagmus and dissociation can unsettle the person and bystanders, so thorough pre‑briefing assists. I have located that calm narration throughout administration reduces the chance the client will certainly stress as the medication takes effect.
Nitrous oxide still shows up at some occasions. It is outstanding for brief, sharp procedures, however logistics and contraindications complicate its use. Expecting individuals, those with digestive tract obstruction, pneumothorax, or entraped gas issues need to not obtain it. Cylinder management at a jampacked site becomes a second risk if not controlled.
Whichever representatives you lug, PUAEME008 anchors practice in clear protocols and extent. Do not improvisate beyond training and authorisation, also when stress installs. If your pain administration training course covered intranasal fentanyl and you work under an agreement that allows it, you get on solid ground. If ketamine is not in your practice design, the best selection is to rise or seek extra support, not to press boundaries.
Non pharmacological Strategies: Commonly Faster, Constantly CheaperI have actually enjoyed a distressed patient's pain decrease pain management training for nurses from eight to 4 within two minutes with absolutely nothing more than a great splint, a cozy covering, and controlled breathing. We talk about drugs due to the fact that they seem like action, yet fundamental steps matter.
Immobilisation and splinting stay the most powerful non‑drug interventions for injury pain. Effectively padded, well positioned splints minimise movement and muscle spasm. Gentle traction in presumed long bone fractures can eliminate the worst of it also before clear-cut treatment. Cold treatment decreases swelling and numbs surface cells when used judiciously. Heat can aid muscle mass convulsion, however avoid it on fresh terrible injuries.
Positioning slides under the radar. A client with kidney stone pain frequently locates alleviation crinkled on one side. Rib fractures really feel much better with the upper body somewhat elevated and supported. Urge settings that reduce muscle mass stress, given back injury is not thought. Easy breathing training decreases considerate drive and enhances tolerance. I use a three matter in, 6 count out rhythm to advertise parasympathetic tone, tuned to the patient's convenience. Include distraction. Led imagery sounds soft up until you see a kid with a forearm crack settle sufficient for cannulation because you asked about their dog and the following soccer match.
Non pharmacological treatment is where physiotherapists and nurses bring substantial worth. Discomfort management programs for physiotherapists frequently stress activity methods that minimize pain without increasing stress and anxiety, and registered nurses bring a second sight for positioning and peace of mind that pays returns. PUAEME008 anticipates responders to demonstrate these steps along with pharmacology, not as an alleviation reward when the medication set is light.
Consent, Communication, and Cultural SafetyConsent can not be a rushed checkbox. Nearly every field mistake I have actually evaluated after an adverse response entailed poor pre‑briefing. Prior to you deliver any analgesia, explain what you plan to do, why, what the person may feel, and what side effects to watch for, then request for permission. Adults with capacity can refuse discomfort alleviation also if you believe it is in their passion. Document the conversation.
Cultural safety issues. Avoid assumptions about pain expression. Some people will certainly underreport discomfort to fulfill perceived expectations. Utilizing neutral, open language aids. As opposed to asking "Is it a 10 out of 10?", try "Can you reveal me on this range how solid the pain feels now?" For Initial Nations clients, invite a support person when possible and be mindful of gendered care choices in some areas. Time invested earning trust is hardly ever thrown away and frequently shortens the total time to effective relief because the person engages with your plan.
Paediatrics and older grownups need unique focus. With youngsters, permission involves moms and dads or guardians, but the child is entitled to an age‑appropriate description and acceptance. Older grownups metabolise drugs in different ways, and polypharmacy increases threat. Halve the first dosage, titrate slowly, and keep a hawk's eye on respiration. I have stood in long transport lines throughout heatwaves where a small second dosage of an opioid tipped a sickly client from comfortable to dangerously sluggish. Protocols frequently permit half doses for older grownups. Use that flexibility.
Monitoring and Managing Adverse EffectsMonitoring is the spinal column of safe analgesia. Document baseline vitals and repeat at intervals matched to the medication's start and optimal. Opioids demand respiration rate and depth checks, oxygen saturation fads, indicators of respiratory tract blockage, and sedation degree. Ketamine asks for blood pressure, heart price, nystagmus tracking, development responses, and nausea or vomiting. Methoxyflurane requires focus to level of consciousness and high blood pressure. Non‑opioid representatives are not freebies. NSAIDs carry GI bleeding and renal stress risk, though these emerge over much longer perspectives. Expect allergic reaction with any kind of agent.
Adverse effects occur, despite having ideal technique. The metric of skills is not staying clear of every occasion. It is recognition and definitive administration. If a patient comes to be overly sedated after fentanyl, quit application, support the air passage, apply additional oxygen, and ready bag‑valve‑mask support. If ventilation is inadequate or oxygen saturation falls in spite of air passage maneuvers, make use of naloxone per procedure. I show students to pre‑calculate the naloxone dosage for their person instantly after carrying out an opioid, and to verbalise the place of the ampoule. Under tension, this small habit maintains your action measured instead of frantic.
Nausea prevails, specifically with opioids and methoxyflurane. Have antiemetics accessible and place a vomit bag in the person's hands. Wooziness and orthostatic decrease in pressure typically settle with placing and liquids, if procedures allow. Keep an eye on the clock. Medicines have half lives, and transportation times can be misleading. If you carry out analgesia right before handover, communicate that explicitly so the obtaining clinician comprehends the timing and can expect the next review window.
Documentation and Handover: The Tale Needs To TravelGood notes make you a far better clinician. Poor ones deteriorate depend on and connection. For PUAEME008, paperwork indicates the discomfort analysis device used and ratings gradually, the medicines administered with dose, path, and time, the person's reaction, unfavorable effects and actions taken, approval discussions, and non‑pharmacological actions. It additionally means context: mechanism of injury, placement discovered, and any type of obstacles or delays.
Handover gain from a basic framework. I favour an adapted IMIST‑AMBO strategy for discomfort: Identification, Mechanism, Injuries/illness, Indications consisting of discomfort scores and vitals, Treatment offered (both non‑pharm and pharmacological), and action. If the obtaining group hears that you titrated 20 micrograms of intranasal fentanyl to a paediatric forearm crack, with pain minimizing from 8 to 3, which the youngster remained sharp with secure vitals and no nausea, they instantaneously understand where to select up.
Training Pathways and Who BenefitsPain monitoring training can be found in different flavours. Short programs hurting administration packaged around PUAEME008 usually run 1 to 2 days, with a balance of theory, simulation, and sensible analysis. Some service providers include optional components like nitrous oxide handling, or sophisticated splinting. A certificate course in pain monitoring at this level does not grant authoritative authority on its own. It verifies proficiency to provide analgesia within an organisation's professional governance and standing orders.
For nurses who pick up changes in occasion medicine or run in country centers, discomfort administration training courses for registered nurses help equate hospital‑based abilities right into prehospital restraints. Focus falls on limited sources, solo decision making, and paperwork that creases efficiently into ambulance or access handover. Physiotherapists functioning pitch‑side or in remote outreach add worth through biomechanics and gentle activity methods. Discomfort monitoring courses for physiotherapists instruct exactly how to couple those toughness with secure analgesic procedures when physicians are not quickly available.
Paramedic pupils usually encounter PUAEME008 integrated into their broader program. For very first responders in the sources sector, a give discomfort monitoring course may be a licensing demand prior to being rostered to solo protection. The pragmatic benefit is clear. When I contrast occurrence records prior to and after staff finish a pain monitoring qualification program, I constantly see faster time to first analgesia and fewer unexpected negative events. The act of practicing authorization manuscripts, rehearsing dosing, and memorising red flags changes practices under stress.
Equipment and Setting: Details That MatterYou do not require a medical facility to deliver great discomfort care, however you do need reputable package and a system that keeps it all set. Stock lists conserve jobs. Inhalers ran out last month assistance nobody. Atomisers that do not fit your syringes thwart strategies. Add human factors. A dark stadium tunnel without a headlamp turns creating medication right into a risky video game. A windy roadside strips heat from a semi‑dressed individual and pushes their discomfort up while you prepare a line. Tiny touches get forgotten up until they attack. I put a thermal covering under and over injury people whenever possible, after that reassess pain prior to I reach for drugs.
Storage and security issue. Opioids need secured storage space and cautious audit. Keep a tamper‑evident system and train every personnel to utilize it similarly. Naloxone ought to sit near opioids, not hidden in a different pouch. I have actually seen groups keep it in an anaphylaxis set two zips far from the fentanyl. During a dilemma, those zips end up being canyons.
Finally, practice where you stand. In confined altering rooms, determine ahead of time who attracts, who holds, that records. Simulation with full equipment is worth an hour of slides. The very first time you try to titrate ketamine while a demonstrator's good friends crowd the entrance needs to not be the first time you understand your monitor cord is too brief for that corner.
Legal and Ethical BoundariesPUAEME008 thinks method within a governance structure. Jurisdictional rules and organisational methods define which agents you can utilize, under what conditions, and with what oversight. Pain monitoring accreditation does not license you to experiment. It confirms you can use a defined procedure securely. Maintain duplicates of your scope of method, standing medication orders, and unfavorable event rise pathway obtainable. If you work throughout organisations, anticipate variation. One employer might permit intranasal fentanyl under a professional technique standard. One more may limit your analgesia to dental representatives and methoxyflurane.
Ethics surface most dramatically when patients decline care, when bystanders press you to rush, or when an associate prompts a shortcut that sneaks beyond protocol. Your support is the combination of individual freedom, educated authorization, and non‑maleficence. Decline to carry out a medicine if contraindications exist, even if the individual firmly insists. On the other side, do not keep analgesia as a bargaining chip for cooperation. Align with the getting service early when you prepare for complex choices. A fast phone get in touch with buys clinical and legal cover.
Building Competence: What Quality Training Looks LikeNot all discomfort monitoring training programs cover the exact same ground. Search for programs that stabilize pharmacology with circumstance time, consist of tools handling drills, and need demo of approval discussions. A good supply pain administration program consists of:
Realistic simulations that evaluate assessment, medicine prep work, tracking, and handover with time pressure. Coverage of non‑pharmacological strategies together with pharmacology, with functional splinting drills. Clear web links to protocols and extent, consisting of paperwork themes and unfavorable event management. Paediatric and older adult factors to consider, with dosing variations and communication techniques. Assessment that consists of duplicated reviews over a circumstance, not simply a single dose and done.As an assessor, I expect the rhythm of care: examine, choose, explain, prepare, carry out, monitor, reassess, record, turn over. When students internalise that loop, their patients get better care and their stress and anxiety goes down.
Common Mistakes and How to Stay clear of ThemA few patterns turn up repetitively. The first is treating pain scores as decor as opposed to as decision supports. If the discomfort continues to be high after an affordable onset period and there are no adverse indicators, titrate. If the pain drops to a moderate degree, pivot to comfort measures and stop dosing. The 2nd is equipment errors: empty atomisers, ended vials, missing filters for inhalers. A pre‑shift checklist avoids most of these. The 3rd is taking too lightly non‑drug choices. Discomfort administration is not a competition to see exactly how promptly you can create fentanyl. Splint early, train breathing, regulate the setting, after that reach for the vial.
The most severe pitfall is bad surveillance. A client who looks "comfortable sufficient" can still move right into respiratory anxiety, particularly in warm, enclosed spaces or during transport when motion lulls them. Develop behaviors that survive diversion. Announce your reassessment times out loud. Ask a colleague to establish a timer on the screen or phone. Compose management times on your handwear cover if you must.

When teams welcome the full range of PUAEME008, scenes really feel various. People relocate from panic to involvement. Extrication times reduce due to the fact that movement injures less. Transportation is calmer, handovers more clear. In audits, you will certainly see fewer outliers in dosing and a smoother spread of pain ratings trending down within 10 to 15 minutes of first contact for modest injury. The very best praise I have obtained after a busy celebration change originated from a receiving nurse: "Your notes tell the story, and the person appears like the notes review."
If you are selecting a discomfort monitoring accreditation training course, concentrate on programs that practice the story from first call to handover rather than those that only teach exactly how to push a medicine. If you manage a team, embed the system into regular skills maintenance. Pain administration training for nurses, physio therapists, and first responders is not a one‑and‑done. Protocols develop and skills plain without use. Quarterly short drills keep the edge.
The heart of PUAEME008 is straightforward. Meet discomfort immediately and respectfully, choose treatments that match the person and the circumstance, view meticulously, and tell the following clinician precisely what happened. Do those points well and you will satisfy the expertise. Much more notably, you will help individuals really feel risk-free once more in minutes that otherwise stretch right into an eternity.