Melasma
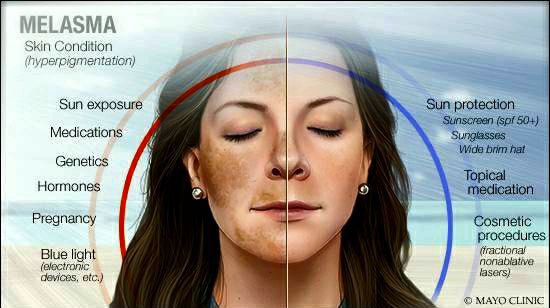
@differential_diagnosis1Melasma is a common, chronic, and recurring disorder of hyperpigmentation arising from hyperfunctional melanocytes that deposit excessive amounts of melanin in the epidermis and dermis. Melasma is particularly common in women, especially those of reproductive age, and in body areas with high amounts of sun exposure, notably the face. Contributing factors involved in the pathogenesis of this condition include genetic influences, sun exposure, sensitivity to hormones, pregnancy, and, in some cases, medications.
Clinical Presentation
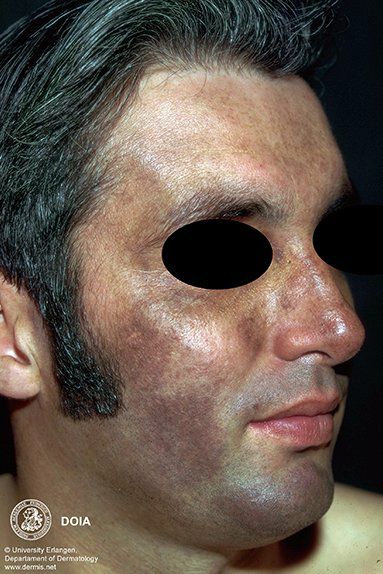
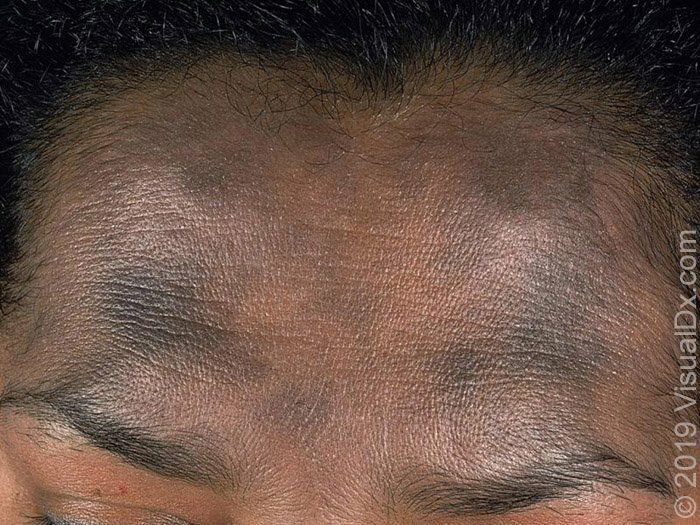
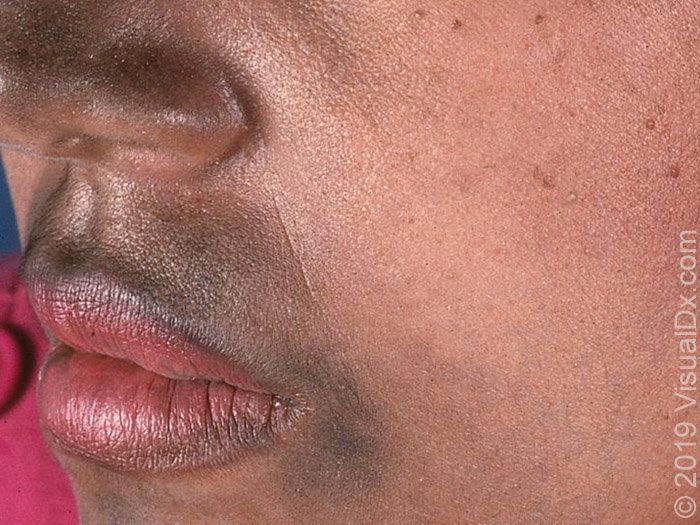
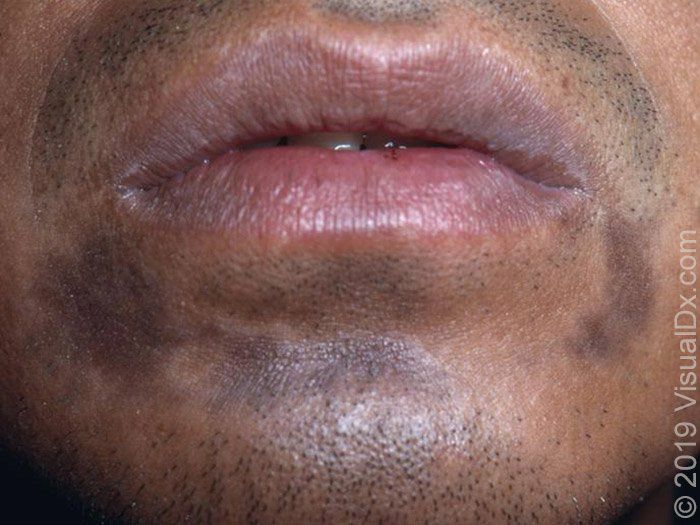
Melasma typically presents with irregular, light-brown to gray-brown macules and patches on sun-exposed skin. The lesions are usually symmetric and may affect the forehead, nose, cheeks, upper lip area, and chin. Common facial patterns of distribution for melasma include the centrofacial, malar, and mandibular forms . Centrofacial melasma commonly affects the forehead, cheeks, nose, upper lip, and chin areas[1] malar predominately involves the lateral cheek areas[2] and mandibular affects the lower jawline[3]

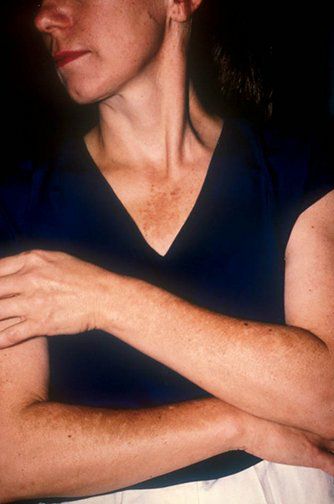
Some patients develop extrafacial melasma, which is less common than the facial phenotype and is usually difficult to treat
Differential diagnosis
🔹️Hori's nevus - Nevus of Hori is a common, acquired, dermal melanocytosis seen in Asian populations, primarily in young and middle-aged Chinese and Japanese women. It presents as multiple speckled, blue-brown or slate-gray macules occurring bilaterally on the malar regions. Hori's nevus is recalcitrant to topical agents used to treat melasma.
🔹️Riehl's melanosis - Riehl's melanosis, also called pigmented contact dermatitis, is a dermal melanosis involving the face and neck caused, in most cases, by chemicals in cosmetics
🔹️Erythema dyschromicum perstans - Erythema dyschromicum perstans is an uncommon, slowly progressive dermatosis characterized by hyperpigmented macules of variable size and shape of an ashen-gray color
🔹️Lichen planus pigmentosus – Lichen planus pigmentosus is a rare form of lichen planus that presents with oval or irregular, brown to gray-brown macules and patches most often located on sun-exposed areas of the skin, such as the face, or flexural areas.
🔹️Fixed drug eruptions – Fixed drug eruption is a cutaneous drug reaction that characteristically recurs in the same locations upon re-exposure to the offending drug. It typically presents with solitary, round to oval, dusky red to brown/black macules
🔹️Discoid lupus erythematosus – Discoid lupus erythematosus lesions of the face may present with postinflammatory hyperpigmentation as well as violaceous hyperpigmentation. However, hyperpigmented lesions are often interspersed with hypopigmented, scar-like areas

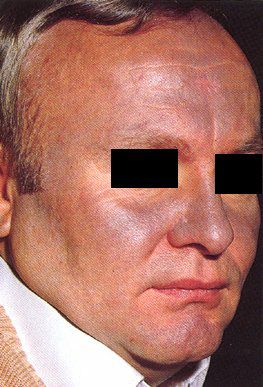
🔹️Phototoxic dermatitis – Phototoxic reactions may occur to a number of systemic drugs, including tetracyclines, thiazide diuretics, fluoroquinolones, and nonsteroidal anti-inflammatory drugs. It usually presents as an exaggerated sunburn limited to the sun-exposed areas that may be followed by postinflammatory hyperpigmentation. Amiodarone may cause a slate-gray pigmentation in a photodistribution of the face
🔹️Phytophotodermatitis – Phytophotodermatitis is a cutaneous, phototoxic eruption caused by the contact with plant-derived substances, such as lemons or limes. It may present with hyperpigmented macules or patches with a bizarre shape corresponding to the areas of contact with the sensitizing substance.
🔹️Postinflammatory hyperpigmentation – Postinflammatory hyperpigmentation manifests as hyperpigmented macules or patches on the skin that match the distribution of the preceding inflammatory dermatosis or injury

🔹️Lentigines – Solar lentigines present with multiple tan to dark brown macules, often with irregular borders. They typically occur in older adults on areas that are chronically exposed to the sun (eg, the face, dorsal hands, extensor forearms, and upper trunk).
