Impetigo
@differential_diagnosis1Impetigo is a contagious superficial bacterial infection with S. aureus and Beta-hemolytic streptococci (primarily group A, but occasionally other serogroups such as C and G) and impetigo observed most frequently in children ages two to five years, although older children and adults may also be affected.
Clinical Presentation
Variants of impetigo include nonbullous impetigo, bullous impetigo, and ecthyma. Systemic symptoms are usually absent. Regional lymphadenitis may occur.
Nonbullous impetigo
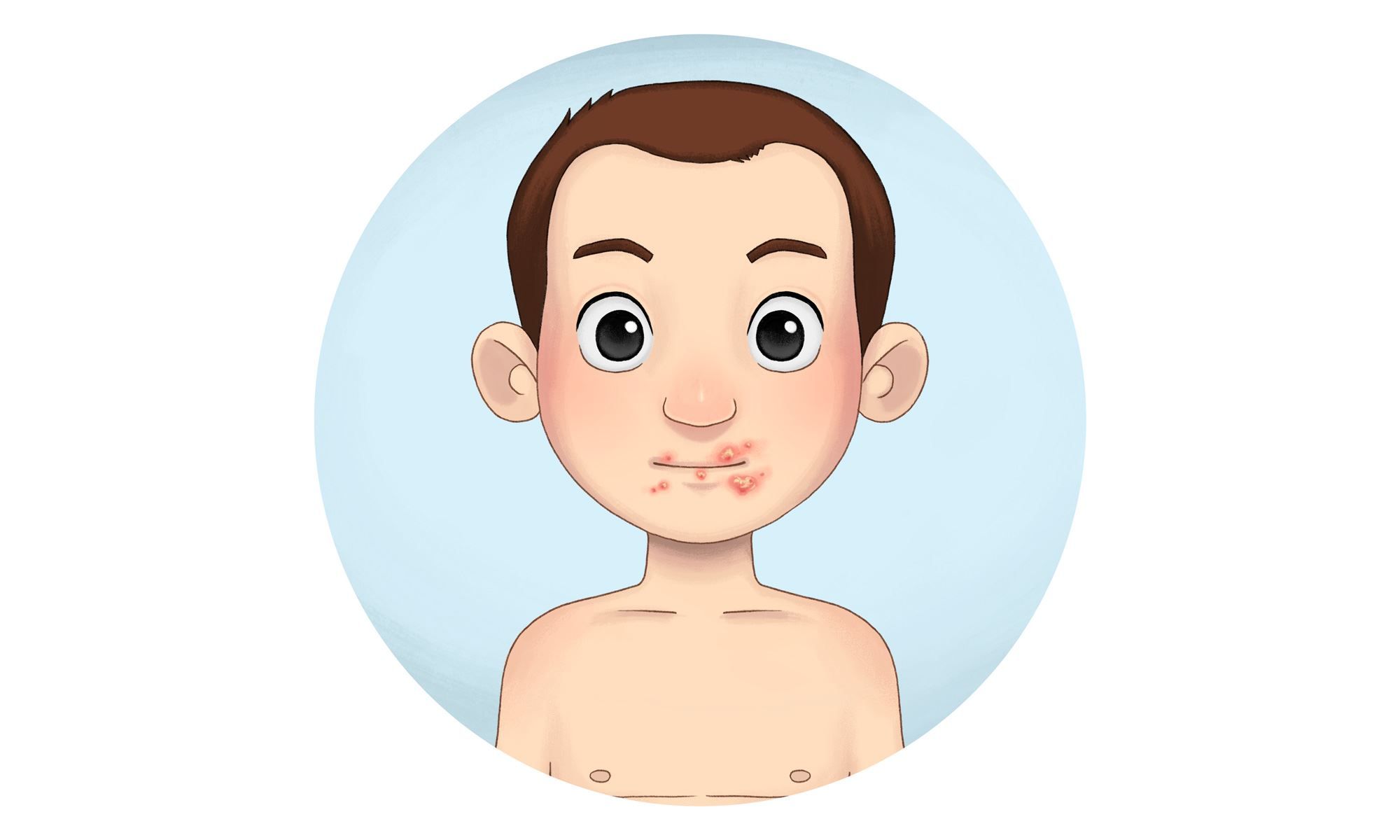
Nonbullous impetigo is the most common form of impetigo. Lesions begin as papules that progress to vesicles surrounded by erythema. Subsequently they become pustules that enlarge and rapidly break down to form thick, adherent crusts with a characteristic golden appearance; this evolution usually occurs over approximately one week. Lesions usually involve the face and extremities. Multiple lesions may develop but tend to remain well localized.

Bullous impetigo
Bullous impetigo is a form of impetigo seen primarily in young children in which the vesicles enlarge to form flaccid bullae with clear yellow fluid, which later becomes darker and more turbid; ruptured bullae leave a thin brown crust. Usually there are fewer lesions than in nonbullous impetigo, and the trunk is more frequently affected. Bullous impetigo in an adult with appropriate demographic risk factors should prompt an investigation for previously undiagnosed HIV infection.
Bullous impetigo is due to strains of S. aureus that produce exfoliative toxin A, a toxin that causes loss of cell adhesion in the superficial epidermis by targeting the protein desmoglein 1. This mechanism is related to the pathophysiology of pemphigus, in which autoantibodies are directed against the same protein.

Ecthyma
Ecthyma is an ulcerative form of impetigo in which the lesions extend through the epidermis and deep into the dermis. They consist of "punched-out" ulcers covered with yellow crust surrounded by raised violaceous margins.

Differential diagnosis
The differential diagnosis of impetigo differs based upon the clinical presentation. Gram stain and culture are useful for confirming the etiologic diagnosis:
● Nonbullous impetigo – Skin conditions that may share features with nonbullous impetigo include a variety of inflammatory conditions that may present with localized areas of inflammation. Examples include contact dermatitis(picture1), tinea infection(picture3), and eczema herpeticum and other herpes simplex virus infections (picture5). Recognition of the characteristic golden crust should raise suspicion for impetigo.
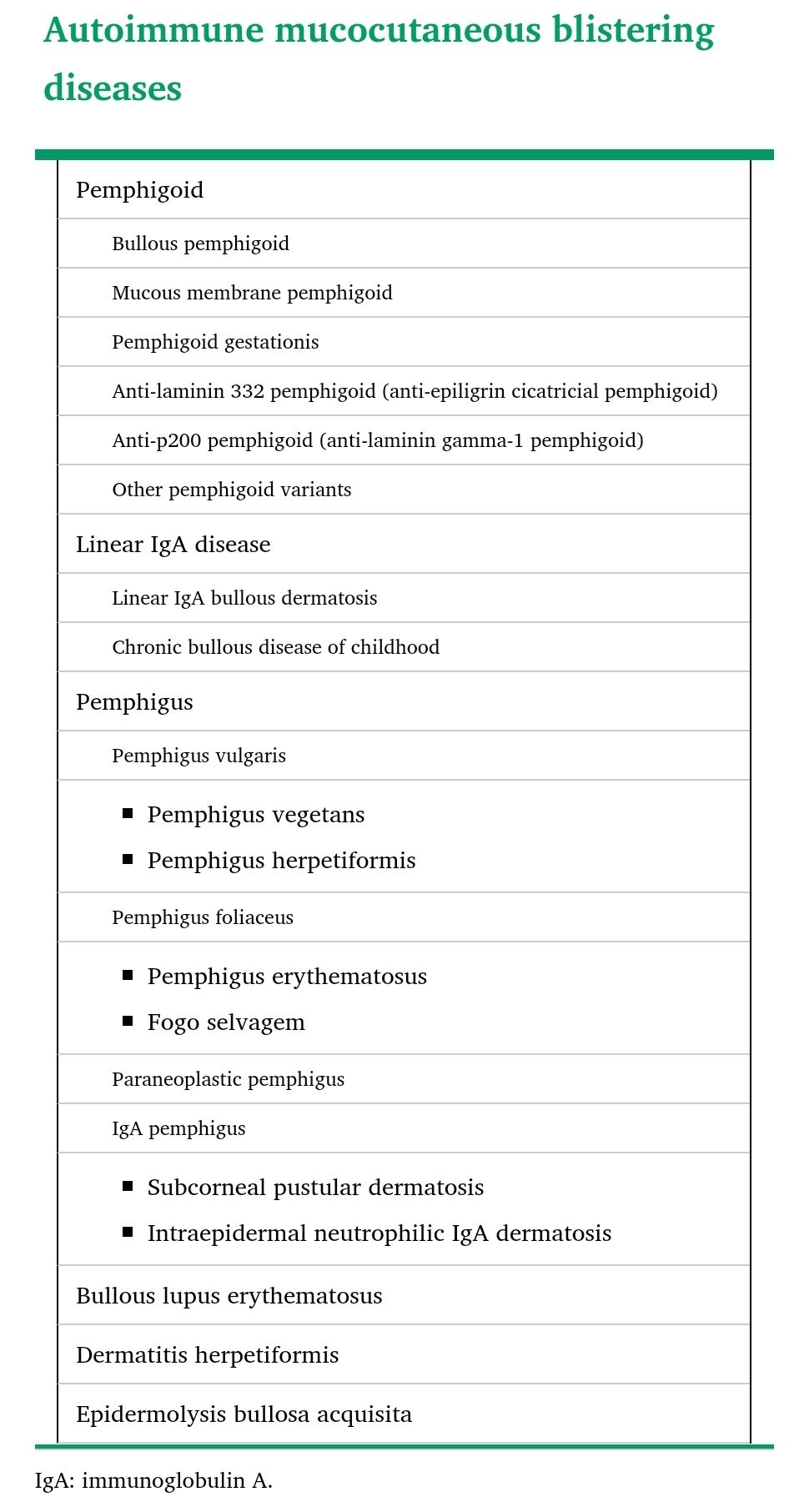
● Bullous impetigo – Bullous impetigo should be differentiated from other blistering skin conditions. Examples include autoimmune blistering diseases (table 1), acute contact dermatitis (picture 7), bullous drug eruptions, burns, bullous insect bite reactions (picture 8A-B), varicella (picture 9), and subcorneal pustular dermatosis (picture 10). The progression from bullae to erosions with peripheral crust is characteristic of bullous impetigo.
● Ecthyma – The differential diagnosis of ecthyma often includes other conditions that may cause localized ulcers, such as mycobacterial or deep fungal infections (picture 11A-B) or pyoderma gangrenosum (picture 12A-B). Ecthyma can be confused with ecthyma gangrenosum, a potentially life-threatening skin condition that occurs in patients with pseudomonal bacteremia. In ecthyma gangrenosum, painless erythematous or purpuric macules rapidly evolve into hemorrhagic vesicles or bullae that subsequently rupture to leave an ulcer with necrotic black eschar (picture 13A-B). Unlike ecthyma, patients with ecthyma gangrenosum are usually systemically ill.
✏ Prescription sample (نسخه) 👇👇
1. Impetigo (نسخه)
Images