Flaccid Hemiplegia
⚡ 👉🏻👉🏻👉🏻 INFORMATION AVAILABLE CLICK HERE 👈🏻👈🏻👈🏻
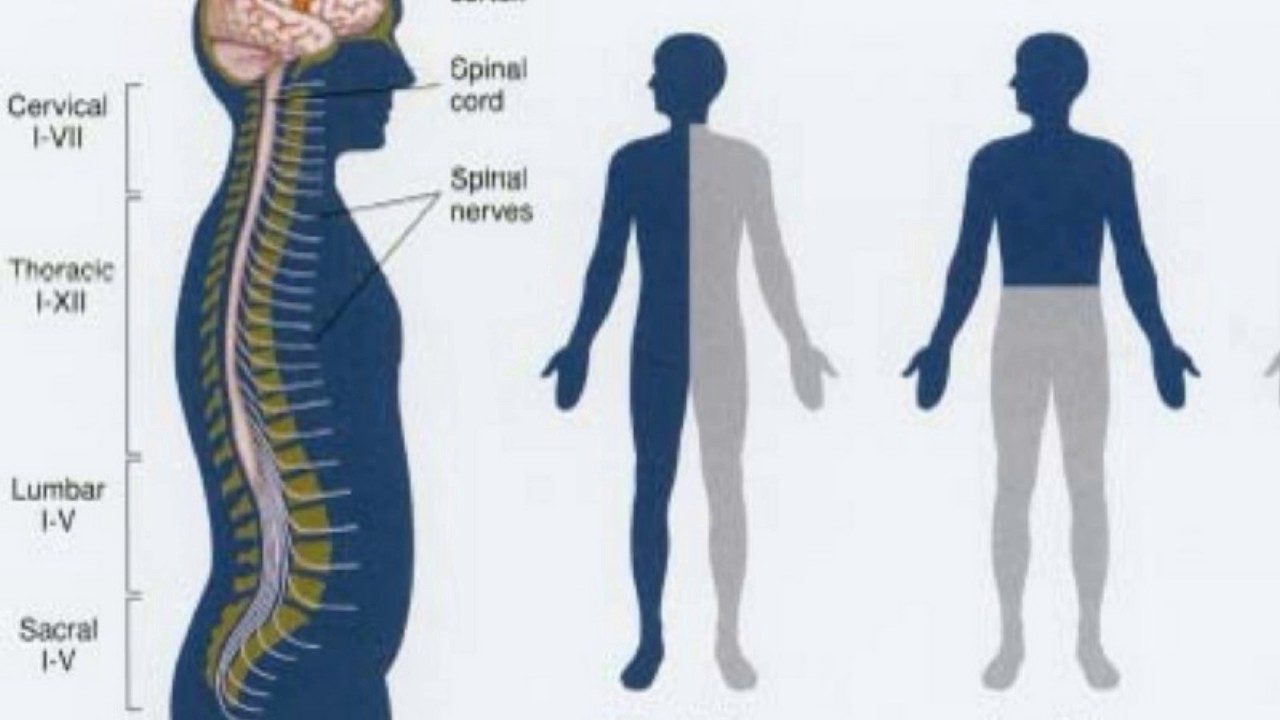
To understand a little hemiplegia we must know that it is a paralysis of the half of the body, usually the compromised side is the opposite of the hemisphere that has been affected by the LCA, this happens because our pyramid route (our information highway) is decided, that is why hemispheric lesions occur on the contralateral side of the body, the exception would be cases where the cerebellum is damaged, where the condition is represented on the same side of the lesion, this happens because the cerebellum is below the decimation of the pyramidal route.
When we talk about hemiparesis, we refer to a notable difficulty of movement, while hemiplegia is a greater degree of difficulty, greatly preventing hand and arm movements in addition to the lower limb, however, both terms are correct, they usually have a healthy side and an affected side, in the upper limb there is a characteristic flexor pattern of the hemispheric lesions, where the advanced or fallen shoulder is observed, the arm meets an elbow flexion, accompanied by pronation or a supination and finally the hand in most cases is closed, in the lower limb the pattern will be extension in the leg, with the hip that rises together with the pelvis, the knee will find it with a problem of flexion , where it is reduced or absent, causing the leg to make a semi-circle movement known as “the biaser’s march” although the latter, it is more common in the condition of the left part, on the other hand, the foot can present with more differences, it can arrive with the first contact on the ground with the fingers, with the lateral edge of the foot or even with the whole plant , all this is because of the alteration of cognitive processes in the affected person that leads to paralysis.
On the other hand, it should be borne in mind that right hemiplegia is a consequence of stroke, which by visible characteristics differs from hemiplegia on the left side; Not only because of the side that is affected by paralysis, it also has specific characteristics that give a remarkable differentiation. There are aspects such as Aphasia (known as a language problem), and also Apraxia are common characteristics of right hemiplegia, however we will see later that when we talk about Apraxia things are a bit different.
One of the most common mistakes in the treatment of this disease and its rehabilitation is to offer a similar or equal therapy for both the right and the left; When we deepen the neurocognitive therapy we realize that each type of injury needs a specific and personal rehabilitation to improve the patient’s quality of life, thanks to this method we have a great tool at hand, even that you can work when the patient is found in the first phase of stroke, which is usually in a wheelchair.
In this disease, the first phase is usually flaccid, this is where all specialists, such as neurologists, neurosurgeons, occupational therapists and physiotherapists, are involved, the faster the paralysis is addressed, the prognosis for recovery is better, but this does not mean If, after the injury has passed, correct work cannot be done for the upper and lower limb involved, remember that the brain is plastic and thus allows a functional recovery despite the time of the disease, now, against This first phase, is caused by the inhibition of all neuronal processes due to brain damage, it is a defense mechanism against massive or partial damage to the brain that is why the patient who is bedridden or in a chair wheels are unable to stand up, can occur anywhere, as well as the cerebral cortex, the basal ganglia, the thalamus, the cerebellum, etc. when there is a marked sagging, usually the patient uses a wheelchair to move around his house or anywhere, this happens because he is unable to walk safely with the lower limb, being the first cause of home care , since this affects the activities of your daily life, starting quickly with neurocognitive therapy in this phase, it is essential that as we move forward in the rehabilitation of the lateral part, there is not a considerable increase in tone in what is known As a spastic stage, this evolution is given by the compensatory mechanisms of the body to be able to generate a movement, it is usually more evident in the hand and foot, but also in the arm and leg, this increase in tone can not only be reached to observer in this case, but also on the left side, depending on the side where the stroke occurred.
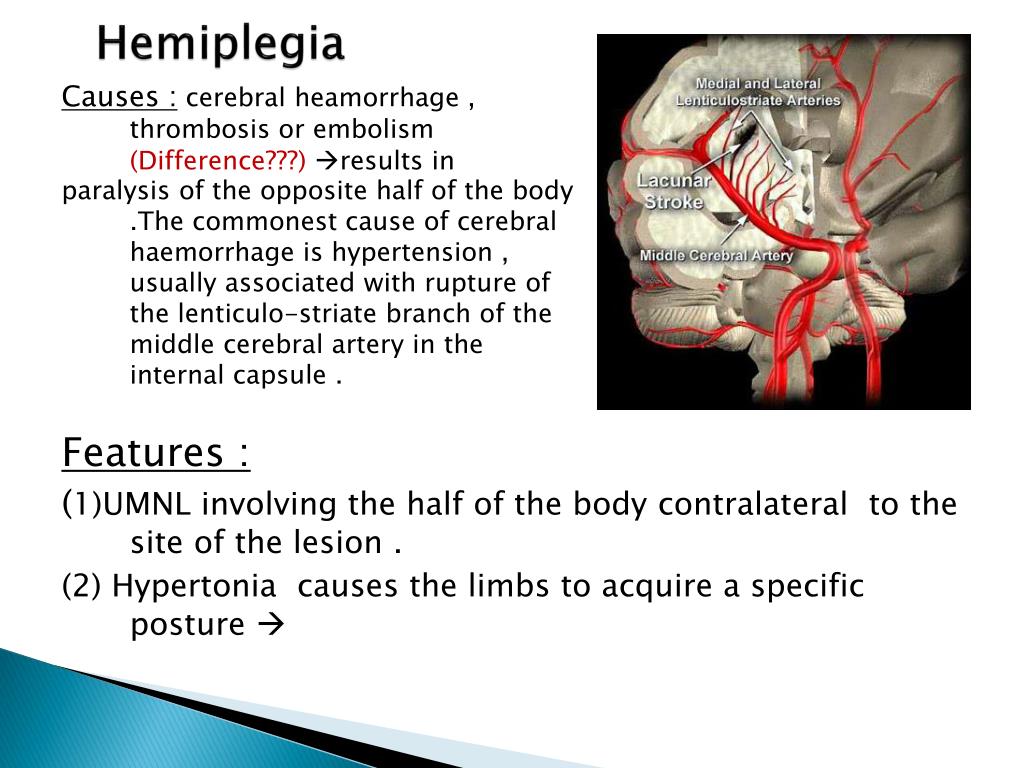
There are generally two types of ACV, it can be ischemic, these are usually produced by any obstruction of the cerebral arteries, known as thrombi, and hemorrhages that are caused by the rupture of these thrombi causing a hemorrhage that touches all parts of the brain that are near the area of the lesion, affecting all the brain areas that come into contact with the lesion focus, even a stroke can occur, but in addition to these, a stroke can be caused by a traffic accident that caused some head trauma, they are usually accompanied by multiple fractures depending on the accident, bruises and in some cases the spinal cord can even be compromised, for something called spinal shock, leaving sequelae not only for an Stroke but also for spinal injury, in other cases also a brain tumor can cause a stroke.
In the first instance, the common element between both lesions seems to be spasticity, which with respect to the healthy side we can observe a great difference in muscle tone, even, this difference may not be so noticeable in certain occasions, but, something that undoubtedly It occurs in most cases is an alteration of movement, a compromise in a series of muscle groups (such as the forearm, hand, knee, foot, etc.) that prevent a movement is generated correctly, but Beyond that, remember that these occur thanks to the complex organization of our mental processes and when we suffer a stroke that affects any area of the brain, as commonly seen in the cerebral cortex, the internal capsule, cerebellum, thalamus, etc; hemiparesis appears due to an alteration of these cognitive processes mentioned above.
In this same order of ideas, let’s interpret the movement and behavior of our body as the tip of an iceberg, we can only observe the tip that would be the movement, but under the water is the great part of this iceberg, which would be the well-organized mental and cognitive processes that consent to its expression.
Obviously a stroke produced by a thrombus that caused a stroke, it can cause ischemia or in the worst case a rupture that causes a hemorrhagic stroke; it alters the ability to organize all these cognitive processes that allow movement; We often hear about different competences of both hemispheres, which participate with different contributions to our motor acts, our behavior and even our language, for this same reason we must always think that there are common characteristics in both lesions, but more markedly there are several notable differences .
What differences can we find in both types of hemispheric lesions?
Surely you have heard that in our left hemisphere is our capacity for language, well, we can say that this is a half truth, I explain myself better, not all our ability to communicate resides in this area, however something we cannot deny is that there is a high possibility that there is a language problem after suffering a cerebral infarction in this area, these language disorders are associated with right hemiplegia, commonly known as: Aphasias.
They will ask themselves: Why does a person suffering from hemiplegia on the right side lose speech? We must consider that language and movement share many cognitive processes, such as attention, memory, among others, so we can define aphasia as the inability to organize communication, remember that language goes beyond saying a word, For example, if we have a dog that is hungry, he will let us know, he may not tell us anything, but his gestures and body language can give us clues about what he wants, now we go with a person who has this problem of language, you may not be able to tell us verbally that you want or need, however, there are other things that can let us know thanks to another type of nonverbal communication.
Aphasia is a much more complex problem for those who deal with rehabilitation and speech therapy, in fact it is confused with the amnesia of words and the mistake is made of asking our patient to repeat any of these over and over again, with the hope that I can remember or learn it; It really is not so, in reality, in most cases, aphasia does not consist of a problem of words, just as hemiplegia does not consist of a problem of muscular contractions, in reality, it is the difficulty of accessing certains rules and forms of language at a given time and context.
When we talk about this type of problems associated with hemiplegia, usually right, this is the result of an alteration of cognitive processes, that is, those such as attention, learning and the ability to make transformations from the body in different informative modalities, as well as language, vision and perception.
Although this is not entirely clear, but this is only a reflection of the complexity of everything that revolves around apraxia, it is often diagnosed with extreme difficulty and treated with occupational therapy in some cases or rarely with specific and supervised therapies to improve the motor problems of the body.
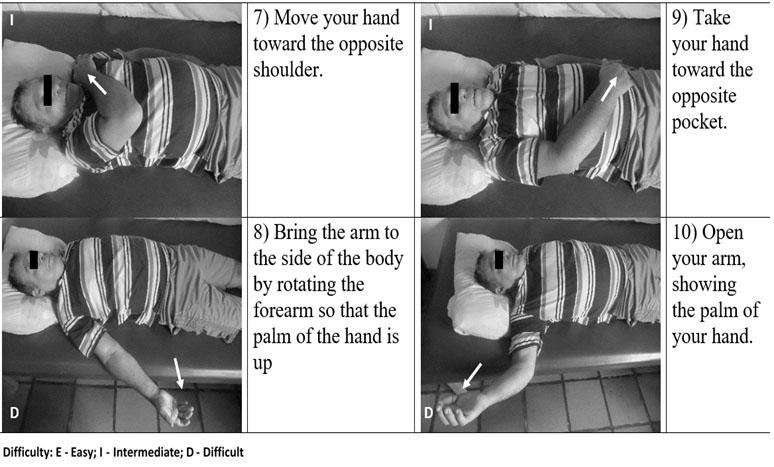
When suffering a hemorrhage or cerebral ischemia that causes a stroke in the right cerebral hemisphere, there are great risks of suffering from apraxia, as we have seen is an extremely complex clinical picture, there are some tests that allow us to show some aspects of apraxia, personally, the one we use the most is the Renzi test, it is simple and easy to use, it is that the patient must imitate a series of gestures that his therapist shows him visually, he must reproduce them with his voluntary movements in the best way and with the least amount of errors possible, all these gestures are made with the unaffected upper limb, they are movements that involve the shoulder, elbow, forearm, wrist and hand, even movements that vaguely involve the head.
In this way, through this test it is possible to select specific characteristics of the Apraxic notes presented in the patient, as we know the right hand and leg are those that are compromised in these cases.
The curious and particular thing about this test is that it makes us reflect on several important aspects, the imitation will always be directed by the left arm, which should have no alteration, no movement problem, but in reality numerous problems of spatial organization are shown, omission of joints that are being used in the gesture, replacement or changes of orientation and even the lack of rhythm in certain repetitive movements of the arm, all these are basic characteristics for a correct motor behavior.
This makes us reflect a little, strokes do not damage the arm or leg, that is, the problem is in the ability to organize the appropriate movement to the context that is required, therefore, in this type of hemiplegia, they are compromised motor aspects in the limb that was not affected, where no movement problems should appear, these small disorders appear.
DISCLAIMER
"The Stroke Therapy Revolution Content is provided for informational purposes only and is not intended as medical advice, or as a substitute for the medical advice of a physician"
LtdPROFESSIONAL CREDITS
2007 to 2008 Lecturer at UCSC Cattolica in Rome, Bachelor in Physiotherapy; “Rehabilitation Methodologies”
from 2008 till now as Professor of “Neurotraumathological Rehabilitation” at "La Sapienza" University of Rome
Your email address will not be published. Required fields are marked *
2020 © Stroke Therapy Revolution Ltd Legal notices - Sales conditions
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Cookie settingsACCEPT
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are as essential for the working of basic...
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are as essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.
When refering to evidence in academic writing, you should always try to reference the primary (original) source. That is usually the journal article where the information was first stated. In most cases Physiopedia articles are a secondary source and so should not be used as references. Physiopedia articles are best used to find the original sources of information (see the references list at the bottom of the article).
If you believe that this Physiopedia article is the primary source for the information you are refering to, you can use the button below to access a related citation statement.
Paralysis of one side of the body due to Pyramidal Tract lesion at any point from its origin in the cerebral cortex down to the fifth Cervical segment ( beginning of origin of cervical plexus ) .
Vascular - Cerebral hemorrhage , Stroke , Diabetic Neuropathy.
Infective - Encephalitis , Meningitis , Brain abscess.
Demylination - Disseminated sclerosis , lesions to the Internal capsule .
Traumatic - Cerebral lacerations , Subdural Hematoma . Rare cause of hemiplegia is due to local anaesthsia injections given intra arterially rapidly , instead of given in a nerve branch .
Psychological - Parasomnia (Nocturnal hemiplegia ).
Damage to the CorticospinalTract leads to the injury on the oppoSite side of the body. This happens because the motor fibres of the CorticospinalTract , which take origin from the motor cortex in brain , cross to the oppoSite side in the lower part of medulla oblongata and then descend down in spinal cord to supply their respective muscles.
Depending on the Site of lesion in brain , the severity of hemiplegia varies.[2]
Cortical signs ( Dysphasia , Apraxia , Cortical sensory loss , Convulsions )
Ipsilateral LMN CN Palsy and contralateral hemiplegia
Weber`s Syndrome - Third nerve palsy and contralateral hemiplegia
Contralateral hemiplegia - Cerebral peduncle
Contralateral rhythmic , ataxic action tremor ; rhythmic postural or holding tremor (rubral tremor)
Fifth nerve and contralateral hemiplegia
Lateral Gaze palsy and contralateral hemiplegia
OppoSite side ( Loss of pain and temperature sensation on the body and limbs )
OppoSite side ( hemiplegia without facial palsy )
An accurate history profiling the timing of neurological events is obtained from the patient or from family members in the case of the unconscious or noncommunicative patient . Of particular importance are the exact time and pattern of symptom occurs . The most common , slowest in hours , wakes up in the morning with weakness , history of TIA , old age is typical with thrombosis . An embolus occurs rapidly with no warning , history of heart disease , younger age group , no progression (maximum deficit occurs at onset) . An abrupt onset with worsening symptoms , history of prolonged hypertension , severe headache described as "worst headache of my life " , altered consciousness , convulsions , vomiting is suggestive of haemorrhage. The patient 's past history , including episodes of TIAs or head trauma , presence of major or minor risk factors and medications , pertinent family history and recent alterations in patient function ( either transient or permanent ) are thoroughly investigated.
The physical examination of the patient includes an investigation of vital signs ( heart rate , respiratory rate , blood pressure , clubbing ) , signs of cardiac decompensation, and function of the cerebral hemispheres , cerebellum , cranial nerves , eyes and sensorimotor system.
Dynamic Gait Index, the 4-item Dynamic Gait Index, and the Functional Gait Assessment show sufficient validity, responsiveness, and reliability for assessment of walking function in patients with stroke undergoing rehabilitation, but the Functional Gait Assessment is recommended for its psychometric properties
CRS-R Coma Recovery Scale Revised is used to assess patients with a disorder of consciousness, commonly coma.
Take a look at our Stroke Outcome Measures Overview for more information
CerebroVascular imaging is the main tool to establish the diagnosis of suspected hemiplegia. Advanced neuroimaging can rapidly indentify the occluded artery and estimate the size of the core and the penumbra.
Computer tomography and MRI scans [4]
For acute care of stroke patients, a number of computed tomography (CT) and magnetic resonance (MR) techniques are essential. Noncontrast CT excludes other causes of acute neurologic defi cits and intracranial hemorrhage. CT and MR angiography can identify intraVascular clots, and the CT angiography source images improve detection of acute infarction over plain CT. Diffusion MRI estimates the size, location, and age of infarcted core more precisely, and perfusion imaging estimates the ischemic penumbra.CT and MR imaging techniques are used to provide four types of information that are essential to the care of acute stroke patients.
1. They establish the diagnosis of ischemic stroke and exclude other potential causes of an acute neurologic defi cit.
2. They identify intracranial hemorrhage.
3. They identify the Vascular lesion responsible for the ischemic event.
4. They provide additional characterization of brain tissue that may guide stroke therapy by determining the viability of different regions of the brain and distinguishing between irreversibly infarcted tissue and potentially salvageable tissue.
When a stroke has been diagnosed, determining the underlying aetiology is important with regard to secondary stroke prevention. Common techniques include:
• ultrasound of the carotid arteries to determine carotid stenosis
• electrocardiogram (ECG) t
Solo Pro 3
Nudist Relax In Hotel Movies
Prime High School Sexy
Anime Hentai Bukkake
Hdefporn Com Sleep Teen Rape Anal Porno
The impact of abnormal muscle tone from hemiplegia on ...
hemiplegia flaccid : definition of hemiplegia flaccid and ...
Right Hemiplegia | Stroke Therapy (R)evolution
Hemiplegia - Physiopedia
flaccid hemiplegia - это... Что такое flaccid hemiplegia?
Hemiplegia Symptoms, Causes, Treatment, Impact on Day-to ...
The effect of arm sling on balance in patients with hemiplegia
Flaccid paralysis - Wikipedia
Как переводится flaccid?
Flaccid Hemiplegia