Case from practice 1
farkhodmd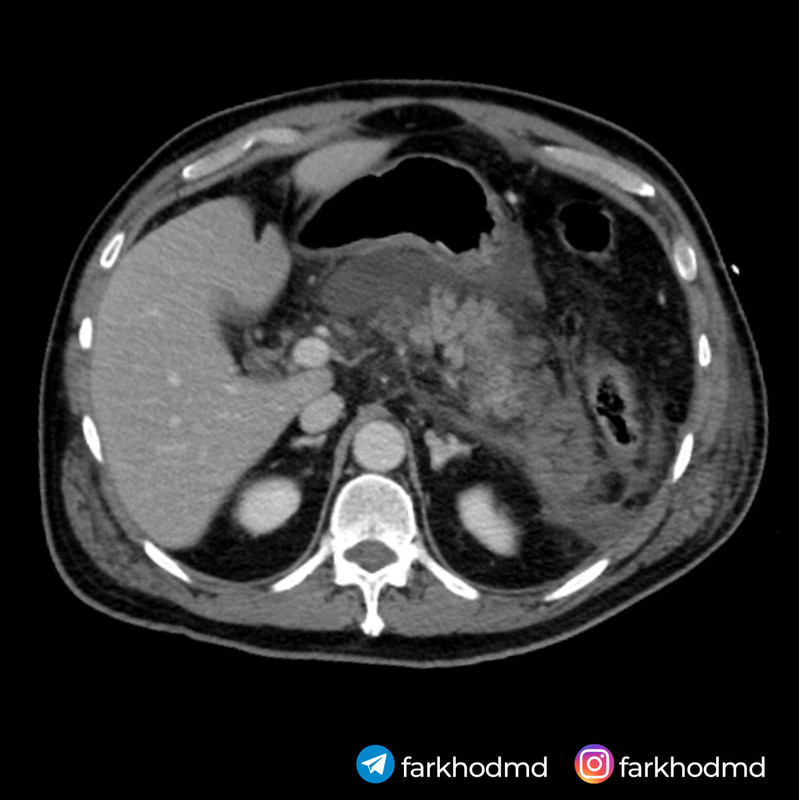
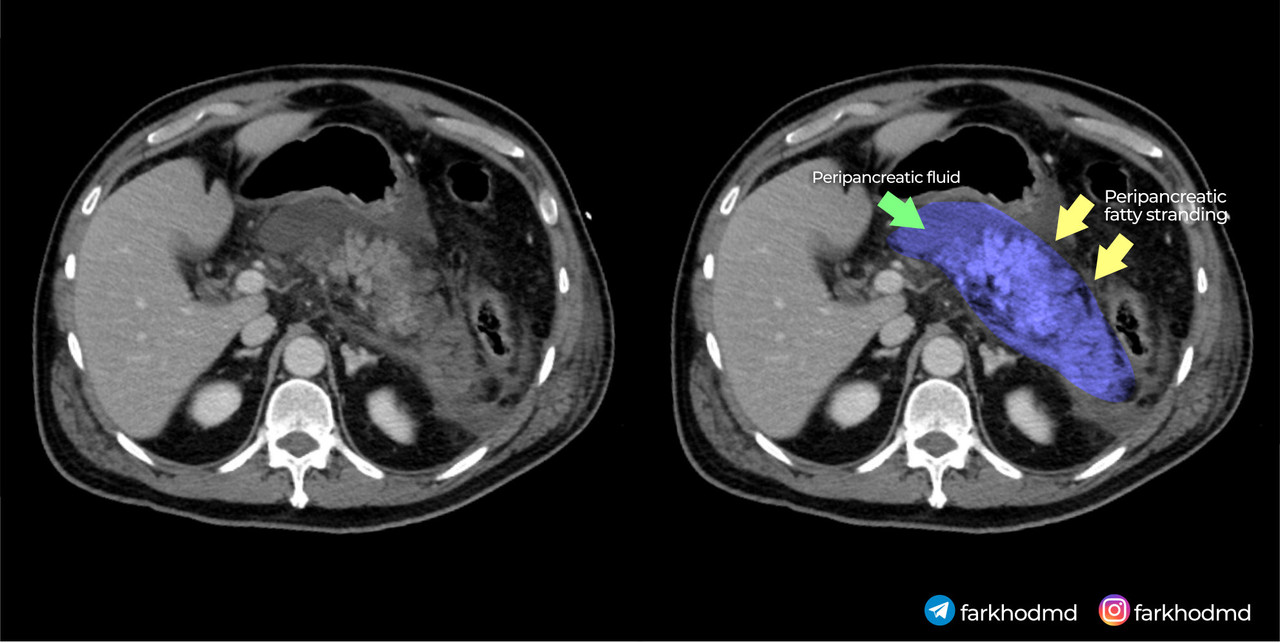
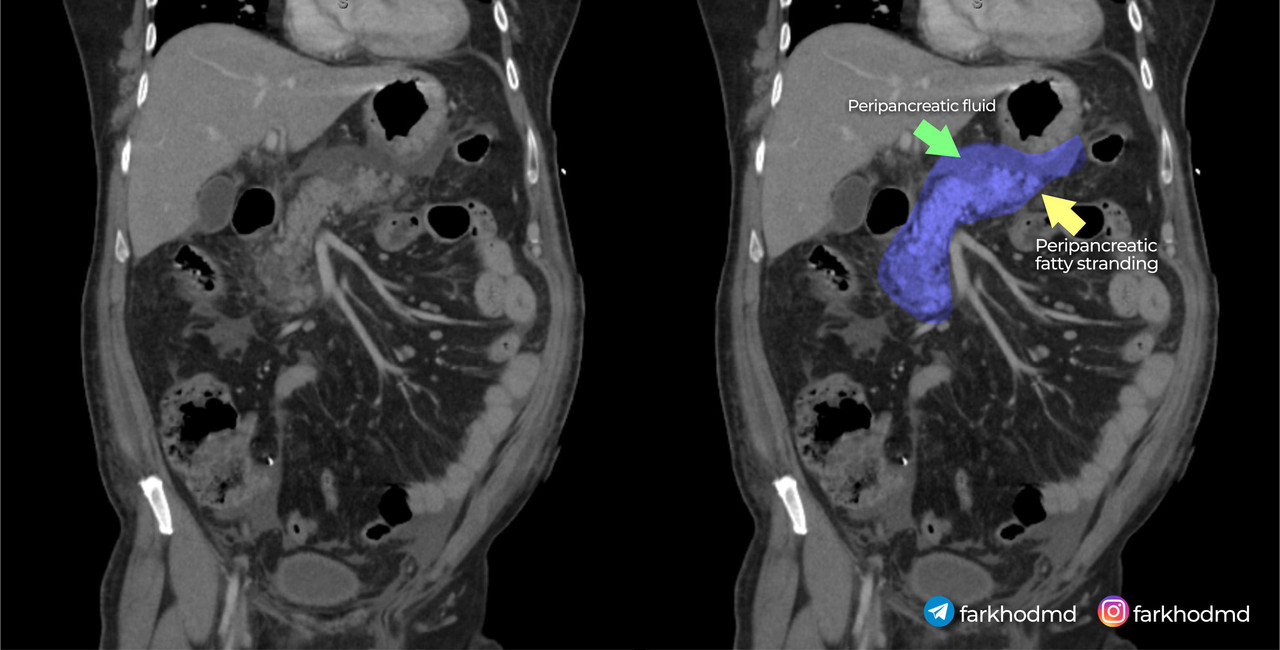
A 56-year-old man with a long history of heavy alcohol consumption presents to the emergency department with severe, persistent epigastric pain that started a few hours after a large evening meal accompanied by multiple beers. The pain radiates to his back, intensifies when supine, and is slightly alleviated by sitting forward. On examination, he appears acutely ill, with mild hypotension, tachycardia, and low-grade fever. His abdomen is markedly tender in the upper region, though without significant rebound tenderness. Laboratory tests reveal markedly elevated serum amylase and lipase. Serum glucose is also elevated. An abdominal CT scan is shown. Despite aggressive intravenous fluid resuscitation, pain management, and supportive measures, the patient rapidly deteriorates and dies within a short period of admission.
Which of the following best describes the underlying mechanism responsible for this patient’s condition?
A. Premature activation of pancreatic enzymes inside acinar cells due to calcium disruption
B. Cystic duct blockage causing gallbladder inflammation
C. Gastric wall perforation leaking acid into the peritoneum
D. Pericarditis causing sharp, positional chest pain
E. Mesenteric artery clot causing pancreatic ischemic necrosis
The correct answer is A: Premature activation of pancreatic enzymes inside acinar cells due to calcium disruption
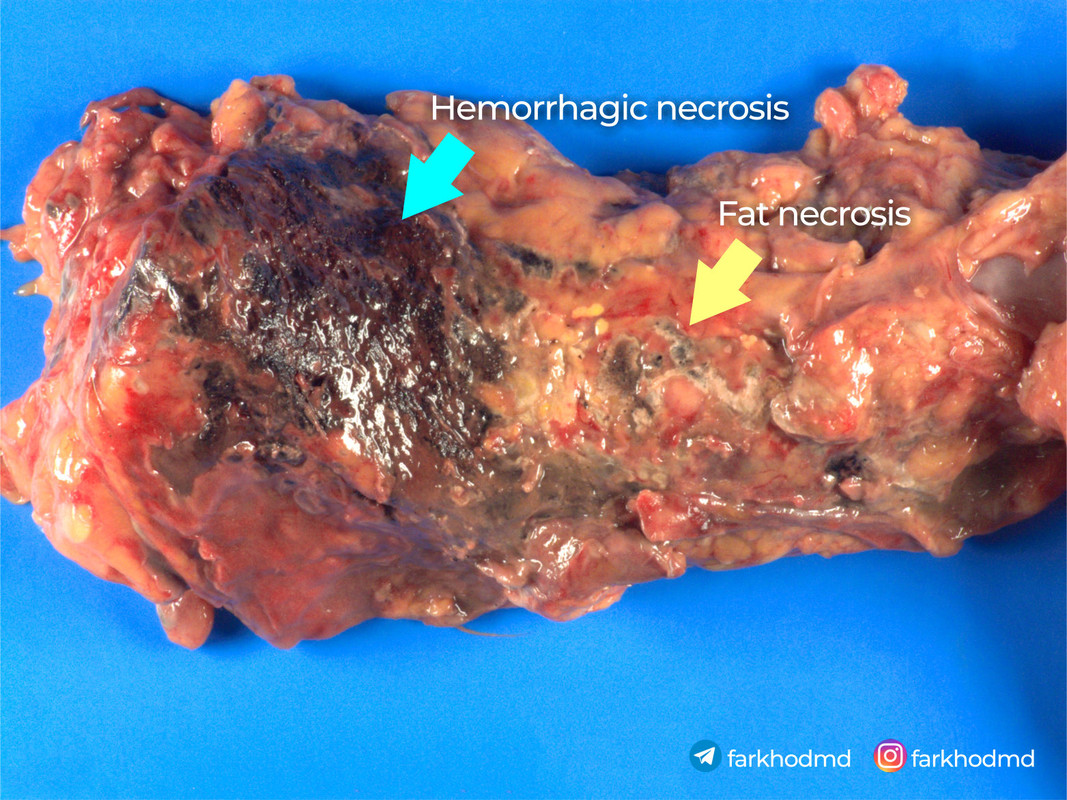
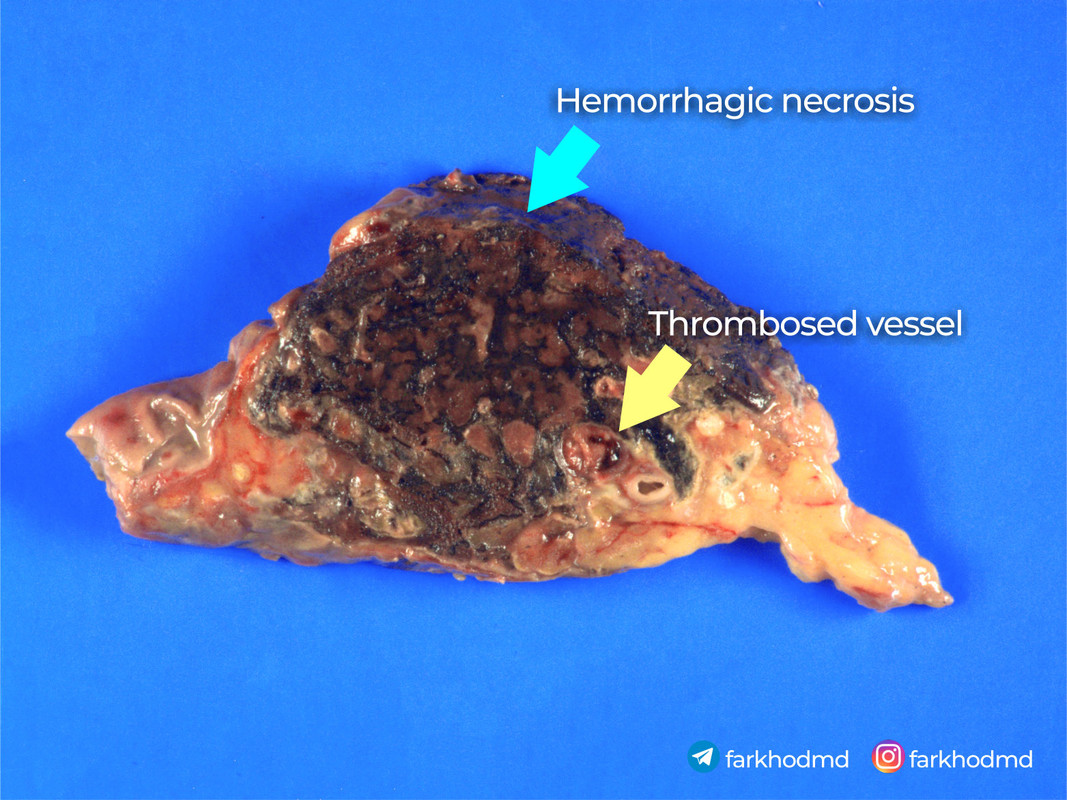
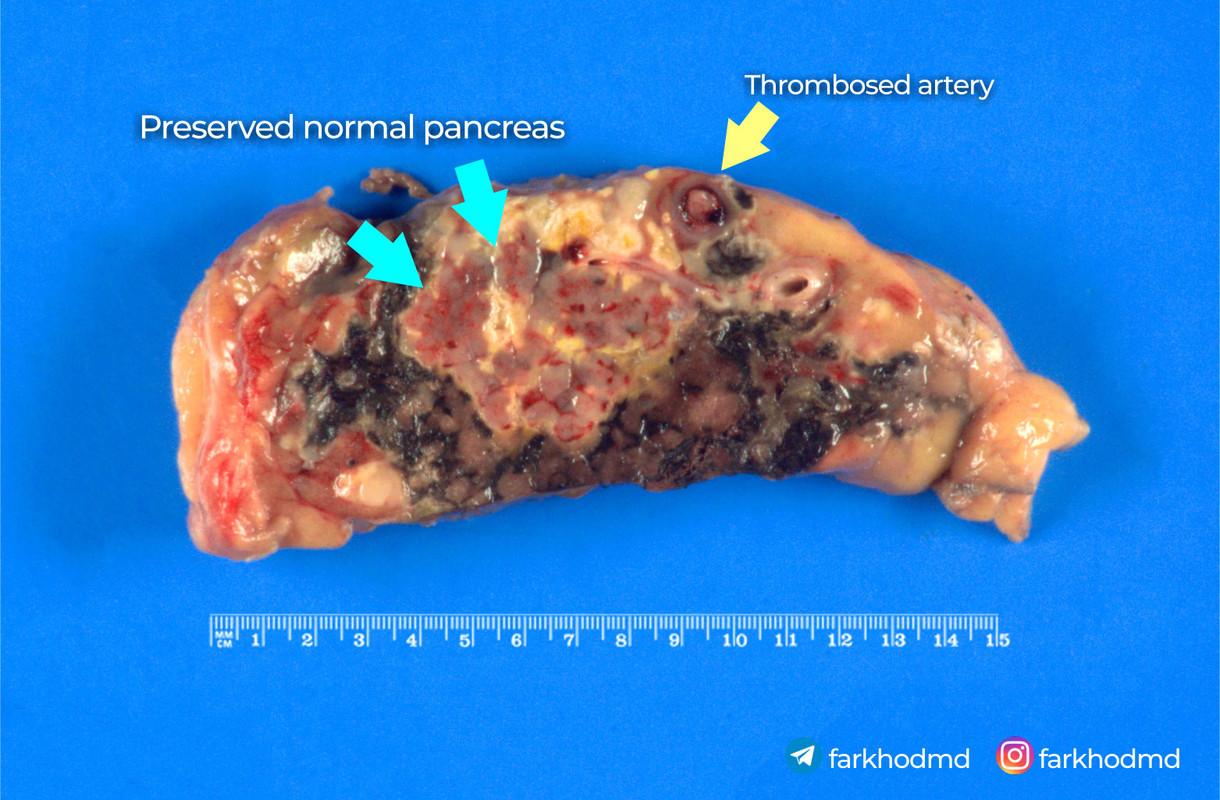
This patient’s presentation, marked by severe epigastric pain radiating to the back, elevated pancreatic enzymes, and hemorrhagic changes on imaging, reflects a severe acute inflammatory process within the pancreas. His longstanding heavy alcohol use sets the stage for pathophysiological alterations in the pancreatic acinar cells. Instead of enzymatic activation occurring normally in the intestinal lumen, the disruption of intracellular calcium signaling leads to premature enzyme activation inside the cell. As these enzymes become active prematurely, they begin digesting pancreatic tissue, causing inflammation, necrosis, and systemic complications. This cascade of intracellular events directly underlies the rapidly progressive and fatal outcome.
Pathogenesis
The key element driving this patient’s condition lies in the disruption of normal intracellular calcium signaling within pancreatic acinar cells. Under physiological circumstances, pancreatic enzymes like trypsinogen are secreted in an inactive form and only become active once they reach the duodenum. In the setting of heavy alcohol use, various factors, including altered intracellular calcium handling, trigger premature activation of these enzymes within the pancreatic acinar cell itself. Elevated intracellular calcium levels lead to the conversion of trypsinogen to trypsin prematurely, setting off a destructive cascade that causes autodigestion of the pancreatic tissue. This enzymatic injury results in necrosis of the acinar cells and subsequent release of proinflammatory cytokines.
These cytokines escalate the local inflammatory response and propagate tissue injury, contributing to systemic inflammatory response syndrome (SIRS) - which the patient most likely died from. As the tissue is digested, hemorrhage can occur due to erosion into blood vessels. Furthermore, damaged acinar cells produce less ATP due to mitochondrial injury, impairing cellular processes and fueling further necrosis. Laboratory evidence includes markedly elevated amylase and lipase, both of which are sensitive indicators of pancreatic injury. Additionally, hyperglycemia occurs due to impairment in insulin regulation when the pancreas is inflamed and damaged.
Therapeutically, management focuses on supportive measures such as aggressive intravenous fluid resuscitation to maintain perfusion and hemodynamic stability, adequate pain control, and careful monitoring for complications. While specific pharmacotherapies may vary, interventions aim to stabilize the patient, prevent complications like infection, and provide supportive nutrition. Research suggests that controlling systemic inflammation and maintaining end-organ perfusion are critical to improving outcomes in severe acute presentations. With prompt recognition and supportive care, some patients recover, but in severe hemorrhagic forms, mortality remains high.
Gross images
Incorrect options
Option B (Cystic duct blockage causing gallbladder inflammation) describes a mechanism underlying acute cholecystitis. While this can present with epigastric or right upper quadrant pain and sometimes mimic other abdominal emergencies, the hallmark typically includes a positive Murphy’s sign, localized right-sided tenderness, and less commonly such profound elevations in amylase and lipase. Moreover, the absence of significant gallbladder abnormalities on imaging makes this less likely.
Option C (Transmural perforation of the gastric wall) suggests a perforated peptic ulcer. This condition often leads to sudden, severe pain and can cause free air under the diaphragm on imaging. Patients typically present with a rigid, board-like abdomen due to peritoneal irritation. In the given case, the absence of pneumoperitoneum or mention of free intraperitoneal air makes this less probable, and dramatically elevated pancreatic enzymes do not generally accompany a simple gastric perforation.
Option D (Inflammation of the pericardium) points to pericarditis. Although pericarditis can present with chest pain that changes with position, it rarely causes severe epigastric pain radiating to the back, nor does it elevate pancreatic enzymes. Additionally, it is less likely to be associated with abdominal fluid collections or hemorrhage within the abdominal cavity.
Option E (Mesenteric arterial thrombosis) would typically present with severe abdominal pain that is often described as disproportionate to physical findings, along with possible altered bowel habits and signs of intestinal ischemia. While it may lead to significant morbidity, it does not typically produce such markedly elevated pancreatic enzymes or a characteristic imaging appearance of pancreatic inflammation and hemorrhage.
By contrasting these mechanisms with the pathophysiology of premature pancreatic enzyme activation, it becomes clear that none of the alternative choices explain the laboratory abnormalities and imaging findings as directly as the correct underlying mechanism.
Outline
The patient’s condition stems from disrupted intracellular calcium signaling in pancreatic acinar cells, leading to premature activation of digestive enzymes. This initiates tissue autodigestion, necrosis, and intense inflammation, with elevated amylase and lipase confirming pancreatic injury. In contrast, other options (cholecystitis, perforated ulcer, pericarditis, mesenteric ischemia) either lack the enzyme elevation or do not align with the clinical and imaging findings. The correct diagnosis explains hemorrhagic changes, severe pain radiating to the back, and rapid deterioration due to systemic inflammatory responses and necrosis.
Interesting fact
Heavy alcohol consumption is implicated in approximately 30-40% of acute pancreatitis cases. It can lead not only to the direct toxic effects on pancreatic acinar cells but also alter the sphincter of Oddi function and increase protein-rich secretions, contributing to ductal obstruction. Chronic heavy drinking predisposes the pancreas to injury, making it more susceptible to episodes of severe, acute inflammation and necrosis.
References
Das SL, Kennedy JI, Murphy R, Phillips AR, Windsor JA. Relationship between Alcohol Consumption and Pancreatitis: A Systematic Review and Meta-analysis. Am J Gastroenterol. 2017;112(7):1043–1051.
Boxhoorn L, Voermans RP, Bouwense SA, et al. Acute pancreatitis. Lancet. 2020;396(10252):726–734.
Scheele GA. Mechanisms of enzyme secretion by the exocrine pancreas. Annu Rev Physiol. 2020;82:43–63.
By Farkhod
https://www.instagram.com/farkhodmd